| |
|
|
INTRODUCTION The pelvis is the central part of the bone
static-dynamic chain which transmits forces of weight, load and
activity. It has its peculiarities: it has the shape of a ring,
built of three flat bones and sacrum, interconnected by strong
ligaments; it has a protective role for many organs and blood
vessels located in the pelvic cavity; integrity and shape of the
pelvic ring play crucial role in load transfer and walking function.
About 3% of all bone fractures belong to pelvic ring disruption (1).
They are caused by high energy mechanical trauma in traffic, fall
from height or hitting a mechanical tool. Pelvic fractures are
rarely isolated, in 60-80% of cases, they occur as part of
polytrauma - they are associated with limb fractures (80-85% of
cases), chest injuries (60%), head injuries (50-60%), abdominal
injuries (in 30%), blood vessel and urogenital tract injuries
(15-20%) (2).
At admission, patients with pelvic ring fractures have two problems:
hemodynamic instability due to blood loss and mechanical instability
due to bone - ligament damage. Vascular lesions and consequent blood
loss are the first complications. Hemodynamic instability and
hypovolemic shock are very common in pelvic bleeding and quickly
lead to death. Hemorrhagic shock is the main cause of death in the
first 24 hours (3). Surgical stabilization of unstable pelvic ring
fracture does not require urgent treatment, but early temporary
stabilization, as the first step of patient resuscitation is
imperative (4,5).
The pathomechanism of pelvic fracture occurance is a consequence of
force applied on the pelvic ring from different directions:
- Anterior - posterior compression of mechanical force
performs external rotation of the wing, pelvic ring opening and
anterior ligaments rupture occur (symphisis pubis and anterior
sacroiliac ligament). If the force is stronger and lasts longer,
it can break pubic bones branches. In this disruption there is
rotational instability and vertical stability.
- Lateral pelvic wing compression is the most common way of
injury. This force compresses or impacts the spongy bone of
sacrum or ileum. These fractures are also not rotatory, but
vertically stable.
- The vertical action of force on the pelvic ring is performed
by pelvic wing movement in vertical direction with rupture of
all ligaments and pelvic floor rupture. These fractures are both
rotatoryand vertically unstable (2,6).
Treatment of pelvic fractures has rules and stages of treatment:
bleeding control, reconstruction and treatment of associated
injuries, and treatment of pelvic ring fractures.
The aim of this paper is to present a case of rotational and
vertical instability of the pelvic ring as a result of a traffic
injury, stages and method of treatment of associated injuries, and
the final surgical treatment and pelvis stabilization.
CASE REPORT
The paper presents a 35 year-old patient who suffered pelvic
fracture in a traffic accident as part of polytrauma (pelvic
fracture, serial rib fracture on the right side of the chest,
urethral rupture). At the time of admission, all resuscitation
measures were taken, the patient was showing signs of hypovolemic
shock (pressure 65mmHg and pulse 95/min). A catheter was placed, and
two venous routes for infusion solutions, analgesics and blood
transfusion were included.
Determining the severity of polytrauma is one of the decisive
factors for determining priority in taking care of the injured, both
at the location of injury and in the trauma centers. To successfully
solve this difficult problem, a large number of scoring systems is
available today, and they are anatomical, physiological or combined.
We have used the Injury Severity Score (ISS), it provides a
numerical description of injuries within polytrauma and represents
anatomical scoring systems. Using this scale, human body is divided
into 6 regions, and with the increase of points, mortality also
increases (7). Our patient had score of 17 points. We also used
Trauma Scor - TS which is a physiological scoring system. It is
composed of Glasgow Coma Scale (GCS) which is reduced by one third
of the value, and assessment of cardiopulmonary functions. It
contains 5 parameters, and the number of points ranges from 1 to 16;
the higher the score, the greater the possibility of the
polytraumatized patient to survive (8). Our patient had a score of
12 points.
To determine the type of pelvic ring fracture, we initially
performed AP radiography and pelvic MSCT. In relation to the
mechanism of injury and position of pelvic ring elements, and
according to Young - Burgess classification (9), the fracture has
vertical sliding of left hemipelvis with rupture of pubic symphysis,
all pelvic ligaments and floor, and sacroiliac joint ligaments, so
the fracture has both rotatory and vertical instability. Strong
mechanical force had a bottom-up direction of action, and caused
rupture and dislocation of pubic symphysis on the left hemipelvis,
as well as fracture of iliac bone in the sacrum area (Scheme 1A, B
and Figure 1).
Scheme 1. Course and direction of mechanical force
that causes hemipelvis sliding in vertical direction. The fractures
are both rotatorily and vertically unstable. A-in young people there
is pubic symphysis rupture, a pelvic floor tear and sacroiliac
luxation, and sometimes a fracture of the pelvic wing. B-in elderly,
there is a pubic symphysis rupture, and due to osteoporosis, pelvic
wing fracture
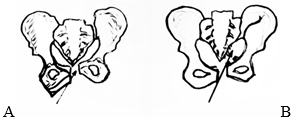
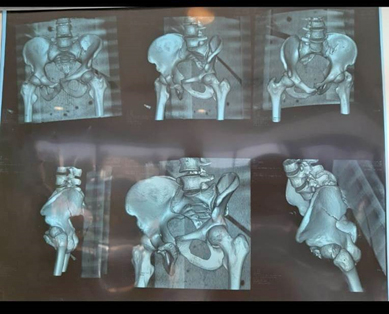
Figure 1. Pelvis MSCT shows left hemipelvis dislocation with
rotational and vertical instability resulting from pubic symphysis
disruption and iliac bone great wing fracture near the sacroiliac
joint.
Urogenital injuries in pelvic fractures are detected by
inspection of external genitalia (labia, penis, scrotum), we monitor
bleeding on the outer opening of the urethra, ability to urinate and
urine color, we examine the perineum, vagina and prostate. If there
is a high displacement of pelvic ring anterior, there is a suspicion
of partial or complete rupture of urethra, so we place a catheter -
if possible. In our case, there is a high displacement, so we placed
a catheter.
During patient follow-up period, an ultrasound examination of
abdomen is performed to detect intra-abdominal bleeding. Hypotensive
patients with positive ultrasound results are an indication for
diagnostic peritoneal lavage. If it is positive (> 8 ml of blood is
aspirated), surgical exploration is indicated (10). In our patient,
the ultrasound abdomen finding was negative.
After complete resuscitation and general condition improvement, on
the third day since injuring, pelvic ring stabilization was
performed. Internal fixation was performed primarily, stabilization
of anterior part with adequate hemipelvis repositioning – traction,
and internal extremities and pelvic wing rotation with radiological
control. A plate was placed over the upper side of the body and
pubic bones branches, and 4 screws were placed over the entire
height of pubic bones body (Figure 2). This way of placing screws
ensures complete stability of the pelvic ring without subsequent
dislocation. Sometimes, for greater pelvic stability, a second plate
is placed at the front of pubic bones. On the fourth day after the
surgery, the patient was discharged, physical treatment was
initiated - sitting and activities in bed, and getting up and
walking with assistance of crutches without support on the left leg
after 2 weeks. Complete recovery and leg support was allowed after 6
weeks.
Figure 2. X-ray after internal pelvic fracture
fixation. The screws were placed over the entire height of pubic
bone body and excellent repositioning and stabilization was
achieved.

DISCUSSION
Pelvic ring fractures can be classified based on mechanical
instability according to Tile classification (A: stable, B:
rotationally unstable, C: vertical and rotationally unstable) (11);
or based on direction and strength of mechanical vector according to
the Young - Burgess classification (lateral compression, antero -
posterior compression, vertical displacement or combined mechanism)
(9).
Pelvic fractures are caused by large mechanical force acting on the
human body, and are always accompanied by bleeding. Bleeding from
spongy bone, presacral venous plexuses and / or iliac arteries and
venous branches, causes hypotension and hemorrhagic shock. Bleeding
is frequent and extrapelvic due to accompanying injuries (chest 15%,
intra-abdominal 32%, long bones 40%). This type of bleeding is the
cause of high mortality in the first 24 hours - more than 40%. In
order to repair hemorrhage, many authors recommend preperitoneal
pelvic packing (12,13).
Pelvic ring stabilization is one of the conditions for stopping
bleeding and hemodynamic restitution, because biomechanical
instability conditions hemodynamic instability, ie. there is a
direct correlation. The external fixation method is often used
(14,15). This method can also be temporary, ie. can be translated
into internal fixation. This procedure reduces intrapelvic volume
and achieves tamponade effect, which leads to the reduction of
bleeding. This way, fracture stability and posterior pelvic ring
elements bone contact is achieved. Many authors recommend primary
internal pelvic ring fixation to achieve both rotatory and vertical
stability (16). In our case, we have also performed internal
fixation of anterior part and thus achieved complete stabilization
and excellent reduction and shape of the pelvic ring.
Urogenital injuries are common in pelvic ring injuries and pose a
risk of infection and death. The result is penetration of a bone
fragment or indirectly due to symphysis diastase (17).
In conclusion, we present experience in treatment of a patient with
pelvic fracture that is both rotatory and vertically unstable. It is
important to assess general condition and bleeding at the time of
admission, as well as to take care of accompanying injuries within
polytrauma, and early stabilization of the pelvic ring fracture.
LITERATURE:
- Durão C, Alves M, Barros A, Pedrosa F. The importance of
pelvic ring stabilization as a life-saving measure in
pre-hospital – A case report commented by autopsy. J Clin Orthop
Trauma. 2017; 8(1): S17–S20. doi: 10.1016/j.jcot.2017.05.011.
Epub 2017 May 30.
- Saveski J. Fracturi na karlica i acetabulum. Skopje, 2002.
- Toth L., King K.L., McGrath B., Balogh Z.J. Efficacy and
safety of emergency non-invasive pelvic ring stabilisation.
Injury. 2012;43(8):1330–1334.
- Buckle R, Browner BD, Morandi M. Emergency reduction for
pelvic ring disruptions and control of associated hemorrhage
using the pelvic stabilizer. Tech Orthop 1994:9:258-266.
- Skitch S, Engels PT. Acute Management of the Traumatically
Injured Pelvis. Emerg Med Clin North Am. 2018;36(1):161-179.
- Tile M. Fractures of pelvis and acetabulum. Baltimore,
Williams and Wilkins, 1995.
- Baker SP, O`Neill B, Haddon Jr W, Long WB. The injury
severiti score: a method for describing patients with multiple
injuries and evaluating emergrncy care. J Trauma 1974;14:187–96.
- Champion HR, Sacco WJ, Copes WS, et al. A revision of the
trauma score. J Trauma 1989;29:623-9.
- Young J.W., Burgess A.R., Brumback R.J., Poka A. Pelvic
fractures: value of plain radiography in early assessment and
management. Radiology. 1986;160(2):445–451.
- Durkin A, Sagi HC, Durham R, Flint L. Contemporary
management of pelvic fractures. Am Journal Surg 2006; 92: 211 –
223.
- Tile M. Pelvic ring fractures: should they be fixed? J Bone
Joint Surg Br. 1988;70(1):1–12.
- Cothren CC, Osborne PM, Moore E, et al. Preperitoneal pelvic
packing for haemodinamically unstable pelvic fractures: a
paradigm shift. J Trauma 2007; 62: 834–9.
- Christopher EW, Joseph RH, John BH. Haemodinamically
unstable pelvic fractures. Injury 2009; 1023–1030.
- Peter BH, Joseph CM, Michael WC. Open fractures of the
pelvis. Review of 43 cases. J Bone Joint Surg 1991;73–B:325–9.
- Majeed SA. External fixation of the injured pelvis. The
functional outcome. J Bone Joint Surg 1990;72(4):612-4. doi:
10.1302/0301-620X.72B4.2380212.
- Leenen LP, van der Werken C, Schoots F, Goris RJ. Internal
fixation of open unstable pelvic fractures. J Trauma 1993; 35:
220 – 5. doi: 10.1097/00005373-199308000-00008.
- Neimi TA, Norton IW. Urovaginal injuries in patients with
pelvic fractures. J Trauma 1985;25(6): 547 – 51. doi:
10.1097/00005373-198506000-00015.
|
|
|
|