|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
Page 39 |
||||||||||||||||||||||||||||||||||||
|
Original paper Analysis of arterial pressure variability by measuring pressure on both arms and as a function of time in patients with newly discovered hypertension Maja Mladenović (1), Zoran Joksimović (2), Igor Đorđioski (1), Anastasija Raščanin (2), Mila Bastać (3), Stanislav Tadić (3), Jasmina Strajnić (3), Dušan Bastać (2) (1) ZAJEČAR HEALTH CENTER; (2) "DR BASTAĆ" INTERNIST'S OFFICE, ZAJEČAR; (3) “MEDSCAN TADIĆ DIAGNOSTIKA” SPECIALIST RADIOLOGY OFFICE, ZAJEČAR |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Download in pdf format | Summary:
INTRODUCTION At the initial office visit, blood pressure should
be measured in both arms, ideally with electronic devices that can
measure them simultaneously. SBP difference between arms >10 mmHg
must be confirmed by repeated measurements. If confirmed, the arm
with the higher blood pressure should be used for all subsequent
measurements, as its values more accurately reflect the level of
blood pressure in the major arteries. Using blood pressure readings
on the arm with higher pressure improves outcome prediction. A
consistent difference in SBP between the arms >15 to 20 mmHg may be
due to atherosclerosis and restriction of the large intrathoracic or
supraclavicular arteries, necessitating investigation of arterial
disease. The blood pressure values on the right and left brachialis
arteries differ in most cases, and the higher one is taken as more
accurate. Prognostic significance: for each 10 mmHg difference
according to Agarwal (2008), the relative risk of total mortality
increases by 24%. In order to accurately assess the degree of
hypertension, the spontaneous variability of pressure as a function
of time and the pressure difference between the arms must be taken
into account. WORK OBJECTIVES: 1. Analysis of spontaneous
blood pressure variability upon arrival and repeated after 5 to 30
minutes; 2. Blood pressure differences between the left (LR) and
right arm (DR). MATERIALS AND METHODS: A prospective study
was conducted from the database of the "Dr. Bastać" Internal
Medicine Practice on 26 patients, average age 58±12 years, with
newly discovered hypertension by measuring blood pressure with the
indirect manometer method at the first examination immediately after
arrival and after 15 minutes. The control group consists of 28
patients who do not have hypertension. The data were statistically
processed with the Student's T test. WORK RESULTS The mean
value (Xsr) of systolic and diastolic blood pressure (SKP/DKP) of
the examined group on arrival is 166/92 mmHg on the right hand (DR),
and 161/93 mmHg on the left hand (LR). and after rest at DR 153/90
mmHg and LR 149/87. There is a statistically highly significant
difference especially between the CAP on the hands - it is always
higher on the right hand by an average of 5 mmHg (p=0.002) and 4
mmHg after rest. Spontaneous variability was determined in 10 (40%)
subjects where there was a statistically significant drop in tension
after rest. After a 15-minute rest, the significance of pressure
differences between arms is maintained, but the high variability of
40% post-rest pressure variability is lost. CONCLUSION:
Pressure on arrival in newly diagnosed untreated patients is always
higher on the right arm by an average of 5 mmHg (p=0.002), and after
rest 4 mmHg, this difference is maintained. Spontaneous variability
was determined in 10 (40%) subjects where there was a statistically
significant drop in tension after rest. After 15 minutes of rest,
the significance of the pressure differences between the arms is
maintained, but the high pressure variability is lost. Key words: Blood pressure measurement/methods, hypertension/diagnosis, hypertension/pathophysiology, arterial blood pressure variability, blood pressure/difference between left and right brachial artery, hypertension/prognosis |
|||||||||||||||||||||||||||||||||||
1. IntroductionAccording to the earlier guidelines and the latest European
guidelines from 2023 as well as international guidelines [1-5], the
definition of systemic arterial hypertension remains unchanged
(short: hypertension) and is defined on the basis of repeated
measurements in the doctor's office: equal to and higher than 140
mmHg for systolic pressure and/or ≥90 mmHg for diastolic pressure.
Arterial blood pressure (BP) is defined just as before as optimal,
normal, high normal or grade 1, 2, or 3 according to the pressure
measured in the office (Recommendation class of evidence I, level of
evidence C) [5]. AIM OF THE PAPER:1. Analysis of spontaneous blood pressure variability on arrival
and repeated after 5 to 30 minutes and METHODS:A prospective study was conducted from the database of the Office of Internal Medicine "Dr. Bastać" on 26 patients, whose average age was 58±12 years, with newly discovered hypertension, by measuring blood pressure with the indirect manometer method at the first examination and control examination 15 days later. The control group consisted of 28 patients who didn’t have hypertension. The data were statistically processed with Student's T test. RESULTSBy comparing the mean values of systolic and diastolic pressures
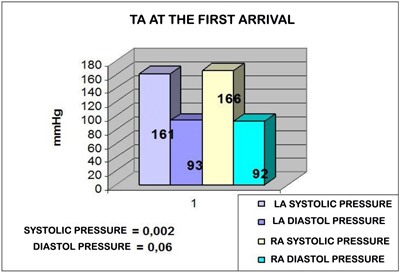
between the arms at the arrival of GRAPHIC 1, we note that there is
a statistically highly significant difference between the SKP on the
arms. The systolic pressure is higher on the right arm by an average
of -5 mmHg (p=0.002), which is maintained even after a 15-minute
rest and then remains 5 mmHg (p=0.001). GRAPH 1. COMPARISON OF SYSTOLE AND DIASTOLE PRESSURES ON THE LEFT AND RIGHT ARMS AT THE FIRST ARRIVAL
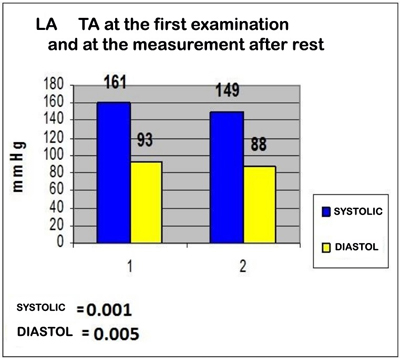
The mean value (Xsr) of systolic and diastolic blood pressure (SKP/DKP) of the studied group on arrival was 161/93 mmHg on the left arm (LR) and 149/88 after rest. (GRAPH 3) which is highly statistically significantly lower pressure after rest: by 12 mmHg systolic (P= 0.001) and by 5 mm Hg diastolic (P=0.005). GRAPH 3. AVERAGE PRESSURE VALUES ON THE LEFT HAND AT THE FIRST EXAMINATION - 1 and at the measurement after rest (CONTROL – 2)
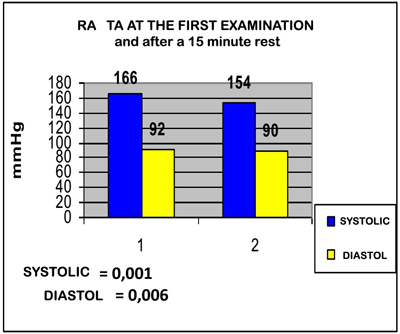
The mean pressure values on the right hand (GRAPHIC 4) are at the
first measurement 166/92 mmHg (GRAPHIC 4). and after rest they drop
to 154/90 mmHg, that is 12 mm systolic pressure and after rest is
statistically significantly lower 12 mmHg (p<0.001), while diastolic
pressure is only 2 mmHg lower without statistical significance
(p=0.06). GRAPH 4. AVERAGE VALUES OF PRESSURE ON THE RIGHT ARM AT THE FIRST EXAMINATION - 1 and after a 15 minute rest (CONTROL – 2)
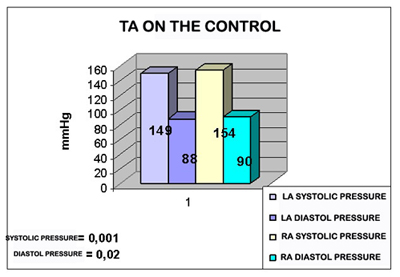
In the individual distribution, blood pressure dropped by >10% in
24%, and by >20% in 16% of patients - high spontaneous variability.
At the follow-up examination, the significance of the differences in
pressure between the arms was maintained. On the contrary, the mean
value of blood pressure at RA was 154/90mmHg, at LA it was
149/88mmHg, and after rest there was no statistically significant
drop in pressure. DISCUSSIONOur results show that the mean systolic blood pressure in the
right arm was significantly higher - by 5 mm Hg at the first
measurement and by 4 mm Hg after rest. According to data in the
literature, the difference in systolic blood pressure values between
the arms was associated with all-cause mortality and with increased
cardiovascular mortality [10,11]. Systolic difference between arms
is associated with increased all-cause mortality, cardiovascular
mortality, and cardiovascular events. Blood pressure should be
measured in both arms during the cardiovascular assessment. A
systolic difference between arms of 10 mm Hg is suggested as the
upper normal limit [11]. CONCLUSIONThere is an extremely statistically significant difference particularly between the systolic pressure on the arms: it is always higher on the right arm by an average of -5 mmHg (p=0.002) and 4 mmHg after rest. This difference is further maintained. Spontaneous variability was determined in 10 (40%) subjects where there is a statistically significant drop in tension after rest. After the introduction of antihypertensive therapy 15 days later, the significance of differences in pressure between arms is maintained, but the variability of pressure after rest is lost. LITERATURE
|
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||