| |
|
|
Introduction Phlebectasia of the internal jugular vein is a
rare clinical entity characterized by isolated fusiform or saccular
dilatation of the internal jugular vein without torsion ( 1 ).
Clinically, phlebectasia of the internal jugular vein manifests as a
cystic, soft, painless, partially compressible, nonpulsatile mass in
the anterior triangle of the neck supraclavicularly anterior to the
anterior border of the sternocleidomastoid muscle, which increases
with the Valsalva maneuver, during exertion, coughing, crying,
sneezing, and spontaneously decreases during rest ( 2,3 ).
It can occur in almost any cervicofacial vein, but most often
affects the internal jugular vein ( 4 ). More often on the right
side, in boys in the pediatric population ( 5 ). The differential
diagnosis of neck swelling that increases with Valsalva maneuver
includes laryngocele or external laryngeal diverticulum, jugular
phlebectasia, brachial cyst, tumor and cyst of the upper mediastinum,
and inflation of the apical bulla of the lung ( 6 ).
The diagnostic modality of first choice is ultrasound examination of
the soft tissues of the neck at rest, and during the Valsalva
maneuver. Magnetic resonance imaging with contrast angiography and
venography of the main blood vessels of the neck is reserved for the
definitive diagnosis of phlebectasia, especially in pediatric
patients ( 7 ).
Surgical treatment is reserved for patients with complications, or
for cosmetic reasons ( 8 ). The decision on the modality of
treatment of phlebectasia of the internal jugular vein in
asymptomatic and some symptomatic patients involves conservative
treatment.
Case report 1:
A 6-year-old boy. He first presented for examination due to swelling
on the right side of the neck, the change appears and increases with
exertion, coughing or crying for the past month. The mother
describes the appearance of a round, soft, painless change in the
lower third of the right side of the neck that she noticed when the
child cried. Initially, the patient was examined by a pediatrician
and an otolaryngologist who, after conducting diagnostics, suspected
phlebectasia of the jugular veins. The patient had no associated
diseases that could be one of the causes of phlebectasia.
Clinical examination did not reveal any change in the neck at rest,
but during the Valsalva maneuver, an oval change of about 3.5x 5 cm
in size appeared in front of the anterior edge of the
sternocleidomastoid muscle in the lower third on the right
supraclavicular side, painless on palpation, partially compressible,
soft consistency, non-pulsatile, the skin above the change unchanged
(Figure 1).
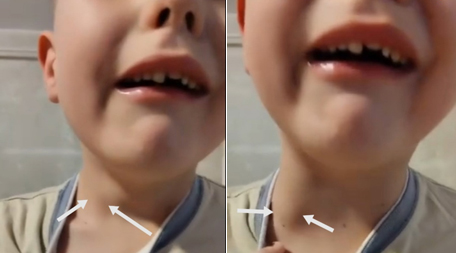
Figure 1: Phlebectasia of the right internal
jugular vein during exertion
Ultrasound examination of the soft tissues of the neck at rest
and during the Valsalva maneuver shows a dilated right internal
jugular vein, without thrombotic masses, without tortuosity. At
rest, the diameter is 12 mm, during the Valsalva maneuver it is 34
mm. The right brachiocephalic trunk is dilated to 7.5 mm. The left
internal jugular vein is up to 7 mm in diameter with regular
characteristics. In hospital conditions, magnetic resonance imaging
of the main blood vessels of the neck with contrast was performed,
which showed an ectatic right internal jugular vein predominantly in
the distal part with a diameter of up to 15 mm, and a left internal
jugular vein with a diameter of up to 7 mm. The jugular veins are
transient, without signs of thrombosis. Due to the benign course and
the absence of complications, the patient was suggested conservative
treatment and a normal lifestyle. Home monitoring and periodic
outpatient check-ups were suggested.
Case report 2:
A 10-year-old boy. He first presented for examination due to a tumor
lesion on the outer side of the right neck, the lesion appearing and
increasing predominantly during exertion for the past six months.
The mother describes the appearance of a round, soft, painless
lesion in the lower third of the right side of the neck that she
noticed when the child was straining. The patient had no associated
diseases that could be one of the causes of phlebectasia. He denies
any other significant complaints (Figure 2a)
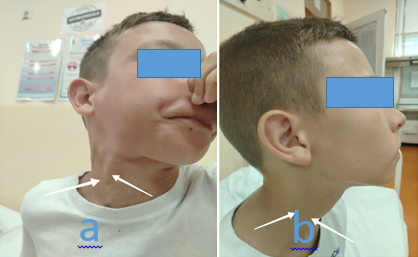
Figure 2: Phlebectasia of the right internal
jugular vein during Valsalva maneuver (a), at rest (b)
Clinical examination at rest does not reveal any changes in the
neck, but during the Valsalva maneuver, an oval lesion measuring
approximately 3 x 4 cm appears in front of the anterior border of
the sternocleidomastoid muscle in the lower third of the right
supraclavicular side, painless on palpation, partially compressible,
soft consistency, non-pulsatile, the skin over the lesion unchanged
(Figure 2b).
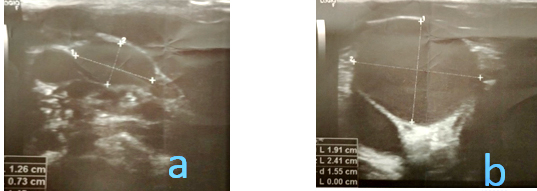
A sound examination of the soft tissues of the neck at rest and
during the Valsalva maneuver shows a dilated right internal jugular
vein, with preserved hemodynamic flow. During the Valsalva maneuver,
the maximum lumen width is 24.1 x 19.1 mm (US Figure 3a), and at
rest, the lumen width is 12.6 x 7.3 mm (US Figure 3b).
Figure 3: (UZ) Ultrasonography of the main blood
vessels of the neck (v. jugularis interna dex.). Cross-section
during Valsalva maneuver (a), at rest (b)
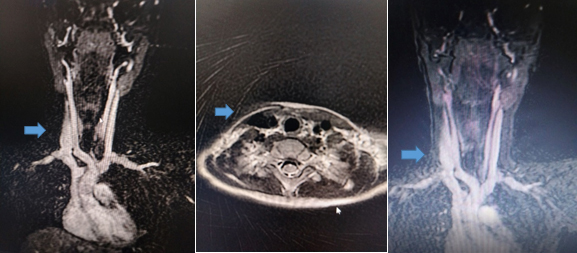
Left internal jugular vein with normal characteristics. In
hospital conditions, magnetic resonance imaging of the main blood
vessels of the neck was performed, which showed that the right
internal jugular vein was wider along its entire length, with a
maximum diameter of up to 11 mm, and the left internal jugular vein
was reduced in diameter to 4 mm. The jugular veins were transient,
without signs of thrombosis (MRI image 4).
Figure 4: (MR) Magnetic resonance imaging with
contrast angiography and venography of the main blood vessels of the
neck - phlebectasia of the right internal jugular vein
Due to the benign course and absence of complications, the
patient was recommended conservative treatment and a normal
lifestyle. Home monitoring and periodic outpatient check-ups were
suggested.
Case report 3:
A 5-year-old girl. The parents report a change in the right side of
the neck in the lower third that increases with exertion. The change
is painless and does not interfere with normal life, and has been
present for the past three years. The patient had no associated
diseases that could be one of the causes of phlebectasia.
Heteroanamnestic data are available on right-sided phlebectasia in a
younger child, also female, in whom the change was seen at birth.
Given the child's early infant age and the fact that the change is
asymptomatic, the child has not yet had a radiological evaluation.
The girl's mother was diagnosed with varicose veins in both lower
legs.
Clinical examination at rest does not show any changes in the neck,
but during the Valsalva maneuver, an oval change of about 2 x 3 cm
in size appears in front of the anterior edge of the
sternocleidomastoid muscle in the lower third on the right
supraclavicular side, painless on palpation, partially compressible,
soft consistency, non-pulsatile, the skin over the change unchanged.
Further diagnostics are recommended, ultrasonography of the soft
tissues of the neck at rest, and during the Valsalva maneuver, as
well as color Doppler of the blood vessels of the neck. It was
explained to the parents that this is most often a benign condition
that requires periodic monitoring in outpatient settings and
parental supervision at home, in case of any complications, surgical
treatment should be considered.
Discussion
Jugular vein flexure was first described by Harris in 1928 ( 1 ),
and anomalous reduplication of the internal jugular vein was
described by Zukschewerdh in 1929 ( 2 ). In 1952, Gerwing coined the
term “phlebectasia” to describe an abnormal fusiform or saccular
dilatation of the vessel ( 3 ).
Internal jugular vein phlebectasia is a rare type of vascular
abnormality characterized by an isolated fusiform or saccular
dilatation of the internal jugular vein without tortuosity. It is
distinguished from varicosity by the absence of tortuosity, and from
aneurysm by the fact that the dilatation uniformly involves the
entire circumference of the vessel.
Clinically, phlebectasia of the internal jugular vein manifests as a
cystic, soft, painless, partially compressible, non-pulsatile mass
in the anterior triangle of the neck, visible supraclavicularly in
front of the anterior edge of the sternocleidomastoid muscle. It
increases with the Valsalva maneuver, during exertion, coughing,
crying, sneezing, and spontaneously decreases during rest. It is
most often asymptomatic and benign, more often affecting boys in a
ratio of 2:1. Dysphonia or aphonia caused by pressure on the
laryngeal nerve is rare, there is a feeling of humming due to
turbulent blood flow in the dilated venous segment, headache,
difficulty swallowing, cough on exertion, shoulder pain,
phlebectasia of the internal jugular vein when moving the right arm,
inability to speak loudly, pain in the root of the tongue, a feeling
of tightness, suffocation and discomfort on exertion, and a feeling
of a foreign body in the neck. Thrombosis, phlebitis, congestive
heart failure, massive bleeding due to traumatic rupture, and
Horner's syndrome are rare (9). Spontaneous rupture of phlebectasia
has not been reported in pediatric patients (10).
Phlebectasia of the internal jugular vein occurs more frequently on
the right side in a ratio of 5.2:1. Bilateral phlebectasia of the
internal jugular vein is less common, somewhat more common in boys
in a ratio of 1.4:1 (11). Possible causes of venous ectasia in the
neck include gross anatomical abnormality, congenital structural
defects in the vein wall, mechanical compression, or trauma, but are
most often idiopathic (12). The most commonly affected internal
jugular vein is the internal jugular vein, followed in descending
order of occurrence by the external and anterior jugular veins, the
jugular bulb, the facial vein, and the superficial communicating
neck veins (13). The more frequent involvement of the right internal
jugular vein is explained by anatomical differences: the shorter
right brachiocephalic trunk, the higher position of the bulb of the
right jugular vein, and the position and size of the valves (14). La
Monte et al. hypothesized that phlebectasia of the internal jugular
vein generally tends to the right because the right brachiocephalic
vein is in close contact with the right apical pleura, and therefore
the increase in intrathoracic pressure could be transmitted to the
right internal jugular vein (15). A venous valve is almost never
observed in the right brachiocephalic vein, in contrast to the left
where the incidence of competent valves is 4 to 8% (16). Paleri and
Gopalakrishnan presented their hypothesis that the increased
intrathoracic pressure is transmitted predominantly to the right
internal jugular vein due to the higher anatomically positioned
valve and larger diameter of the right internal jugular vein, the
shorter right brachiocephalic vein that follows the course of the
superior vena cava, the greater number of competent valves in the
right subclavian vein, and the greater number of valves in the left
brachiocephalic vein (17). Other possible less likely causes include
tracheomalacia and tracheoesophageal fistula, exposure to elevated
positive intrathoracic pressure, internal jugular vein cannulation,
internal jugular vein duplication, congenital primary weakness of
the venous muscular layer, or loss of normal connective tissue of
the vein wall. An association between internal jugular vein
phlebectasia and Menkes disease has been suggested (18).
Histopathological studies have shown loss of the elastic layer and
hypertrophy of connective tissue with focal intimal thickening.
Histologically, diffuse fibrosis and disrupted elastic tissue
architecture suggest a mechanical effect (19). Histopathological
studies of surgically removed specimens show a normal varicose vein
pattern in most cases, but in some cases there is loss or disruption
of the arrangement of smooth muscle cells, elastic fibers, and
connective tissue (20). In 1962, after surgical removal of a
phlebectatic portion of the internal jugular vein, Leighton observed
that smooth muscle fibers were randomly distributed in the vessel
wall and that there was an island of adipose tissue extending into
the tunica intima between the fibers. He called the phlebectasia a
vascular hamartoma (21).
Ultrasonography is the diagnostic modality of first choice, the
diagnosis of phlebectasia of the internal jugular vein is confirmed
by the variation in size during rest and during Valsalva maneuver -
anteroposterior diameter of more than 15 mm. During Valsalva
maneuver, the diameter of the affected vein can increase up to 2.2
times compared to the measurement during rest (22). Color Doppler
ultrasonography confirms the presence or absence of thrombosis in
the vein lumen. Neck and chest radiography, magnetic resonance
imaging of the main blood vessels of the neck and contrast-enhanced
computed tomography additionally provide even more information about
the size of the lesion, anatomical relationships with other
structures, and are indispensable for the definitive diagnosis of
phlebectasia of the internal jugular vein, especially in pediatric
patients (7). Chest and neck radiography can raise suspicion of
laryngocele, or exclude the presence of air, as well as changes in
the upper mediastinum. Laryngoscopy is recommended to complete the
diagnosis and confirm the diagnosis of laryngocele. Invasive
diagnostic radiological procedures and surgical explorations are
rarely used in children, as noninvasive diagnostics confirm the
diagnosis of internal jugular phlebectasia.
The diagnosis of cystic neck swelling is challenging, and the
differential diagnosis in pediatric patients is broad, and in
addition to phlebectasia, it includes: laryngocele, external
laryngeal diverticulum, brachial cyst, cystic hygroma, cavernous
hemangioma, tumors and cysts of the upper mediastinum, inflation of
the pulmonary apical bulla, thyroglossal duct cyst, dermoid cyst,
cervical adenopathy (23). The most common cause of a neck mass that
increases with the Valsalva maneuver is laryngocele, but in
children, phlebectasia of the internal jugular vein should also be
considered ( 6 ).
Phlebectasia of the internal jugular vein increases in size in
childhood until puberty, after which it spontaneously decreases. In
asymptomatic and partially symptomatic phlebectasias, due to the
benign, or self-limiting nature of the disease, the recommended
treatment modality is conservative treatment with regular monitoring
at home and periodic check-ups in a tertiary health care
institution, most often lifelong (23).
Symptomatic phlebectasia of the internal jugular vein with
complications such as thrombosis, compression of vascular
structures, Horner's syndrome, or signs of rupture of the varicose
vein are indications for urgent surgical intervention (24). Surgical
treatment includes ligation of the varicose vein, resection of part
of the phlebectatic venous wall, longitudinal venous constriction
suture, coating and fixation of the varicose vein with the omohyoid
muscle or an 8mm polytetrafluoroethylene tube - PTFE. (25). Cases of
right-sided internal jugular phlebectasia that were treated
surgically have been published, the treatment modalities are shown
in the table ( Table 1 ).
Table 1: Review of world literature - right-sided
phlebectasia of the internal jugular vein.
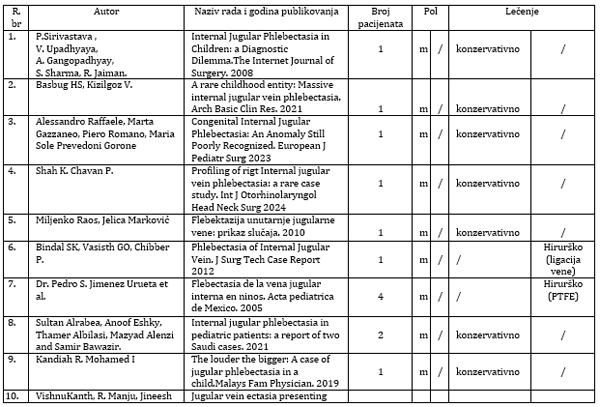 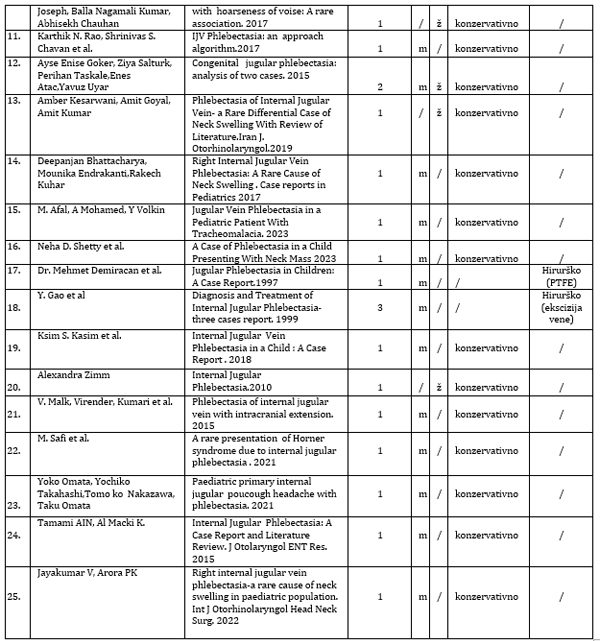
* polytetrafluoroethylene tube- PTFE
Conclusion
Phlebectasia of the internal jugular vein should be included in
the differential diagnosis of atypical neck masses in children. It
can be easily diagnosed with a detailed history and physical
examination. The diagnostic modality of first choice is ultrasound
examination of the soft tissues of the neck at rest, and during the
Valsalva maneuver, because it can be easily and effectively used for
monitoring, so that the extent of the swelling can be documented.
Magnetic resonance imaging with contrast angiography and venography
of the main blood vessels of the neck is reserved for the definitive
diagnosis of phlebectasia, especially in pediatric patients. After
diagnosis, the patient should be followed up regularly. Inform the
patient and his parents about the risk of possible complications.
Most importantly, the patient and his parents should be reassured
that this is most often a benign condition, and that it will not
affect the normal life regimen. The presented patients correspond to
the largest number of patients presented in the world literature in
terms of clinical characteristics, diagnostic method and proposed
treatment modalities.
Literature:
1. Harris RL. Congenital venous cyst of mediastinum. Ann Surg
1928;88:953-6.
2. Zukschwerdt L. Seltene localisation einer venectasie. Ditsch Z
Chir 1929;216:283-285.
3. Gerwing WH Jr. Internal jugular phlebectasia.Ann Surg
1952;135:130-133.
4. Sander S, Elicevik M, Unual M, et al. Jugular phlebectasia in
children: is it rare or ignored? J Pediatr Surg 1999;34:1829-1832 .
5. Dhillon MK, Leong YP. Jugular venous aneurysm – a rare caue of
neck swelling. Singapur Med J. 1991;32(2):177-178.
6. Jianhong L, Huewu J, Tingze H. Surgical treatment of jugular vein
phlebectasia in children. Am J Surg 2006;192:286-90.
7. Miljenko Raos, Jelica Marković. Flebektazija unutarnje jugularne
vene: prikaz slučaja. Med Jad 2010;40(3-4):103-106.
8. Kuo WR, Chien CC, Choi CY et al. Internal jugular phlebectasia.
1992;8:503-9.
9. Figueroa Sanchez J. A. et al. Internal jugular phlebectasia a
systematic rewiev. Surg Neural Int. 2019;10:106.
10. Indudharm R, Quah BS, Swaib IL. Internal jugular phlebectasia-an
unusual case of neck swelling.Annuals of Tropical Pediatrics
1999;19(1)105-8.
11. Kim SW, Shay JW, Lee S. Unusal presentation of a cervical mass
revealed as extended jugular venous aneurysm. Vasc Specialist Int.
2016;32:205-7.
12. Stivens KE, Price JE, Marko J, Kalor SG. Neck masses due to
jugular venous ectasia. Child's Neur Syst. 1995;11(9):533-535.
13. PaleriV, GopalakrishnanS. Jugular phlebectasia: theory of
pathogenesis and rewiev of literature. J Int Pediatr
Othorynolaringol 2001;57:155-9.
14. La Monte et al. Internal jugular phlebectasia. A
clinicoroentgenographic diagnosis. Arch Otolaryngol. 1976;102:706-8.
15. Yokomori K et al. Internal Jugular phlebectasia in two
siblings.Manometric and histopathological studies of the
pathogenesis. J Pediatr Surg.1990;25:762-5.
16. Kwok LL, Lam HS, Ho DKK. Unilateral right-sided internal jugular
phlebectasia in ashmatic children. J Pediatr Child Health.
2000;36:517-519.
17. Leighton JE. Jugular phlebectasia . Postgraduate Medline
Journal. 1962;470-73.
18. Eksioglu AS, Senel S, Cinar G, Karacan CG. Sonographic
measurment criteria for the diagnosis of internal jugular
phlebectasia in children. J Clin Ultrasound. 2013;41:486-492.
19. Hsou Chin C et al. Ultrasonographic diagnosis and color flow
doppler sonography of Internal jugular venous ectasia in children. J
Ultrasound Med 1999;18:411-416.
20. Rosi A, Tortori- Donati P. Internal jugular vein phlebectasia
and duplicationa case report with magnetic resonance angyography
features. Pediatr. Radiol 2001;31(2):134.
21. Rajandran UR, Vasu CK, Regi G, Anja MA, Anoop P. Unilateral
internal Jugular phlebectasia. Indian J Pediatr 2004;71:751-753.
22. Bowdler DA, Singh SD. Internal Jugular phlebectasia. Int J
Pediatr Otorinolaryngol 1986;12:165-71.
23. Blindal Sk et al . Phlebectasia of internal jugular vein. J Surg
Tech Case Rep 2012;4(2):103-05.
24. M. Safi et al. A rare presentation of Horner's syndroms duo to
internal jugular phlebectasia. JAAPOS ( 2022 )
25. Hung T, Campbell A. Surgical repair of left internal jugular
phlebectasia. J Vasc Surg 2008;47:1337-8. |
|
|
|