|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
Page 132 |
||||||||||||||||||||||||||||||||||||
|
Case report Complications in the treatment of segmental tibial fractures Zoran Golubović (1), Predrag Stoiljković (1), Ivan Golubović (1), Milan Pejčić (1), Milan Lazarević (1), Mihailo Ille (2), Ivana Golubović (1), Ivan Milošević (2), Nebojša Mitić (3), Dejan Tabakavić (3) (1) CLINICAL CENTER NIŠ; (2) CLINICAL CENTER BELGRADE; (3) CLINICAL CENTER KOSOVSKA MITROVICA |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Download in pdf format | Summary: Segmental
tibial fractures belong to the group of the most severe fractures of
the locomotor system. They are most common in polytraumatized
patients. Treatment of segmental tibial fractures can be
conservative or operative. Treatment of segmental tibial fractures
is accompanied by a number of complications, such as delayed
healing, dislocation of fragments in one or the other fracture
point, healing of fractures in poor position, non-healing of
fractures, aseptic and septic pseudoarthrosis, infection around
fixator wedges, wound infection of open segmental tibial fracture,
iatrogenic infection, osteomyelitis, and limb amputation. The paper
presents a female patient with a severe segmental tibial fracture on
two levels, who was treated with external skeletal fixation. Without
opening the fracture point, repositioning was performed in the
proximal and distal part and the fractures were stabilized with an
external skeletal fixator. After the operation, the patient was
activated with underarm crutches with relief support on the injured
leg. For the purpose of stimulating fracture healing, low molecular
weight heparin, Fraxiparine (to prevent thrombosis and pulmonary
thromboembolism) and Forticolinn were prescribed. After the fracture
healed, the external skeletal fixator was removed and the patient
returned to her working and living activities. At the follow-up
examination five years after the segmental tibial fracture, the
patient had a stable and firm support on the injured leg. Key words: Segmental tibial fracture, external skeletal fixator, fracture stabilization, prevention of pulmonary thromboembolism, delayed fracture healing, five-year follow-up |
|||||||||||||||||||||||||||||||||||
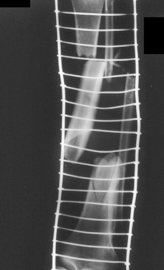
INTRODUCTIONSegmental tibial fractures represent a break in the continuity of the bone tissue of the diaphysis of the tibia at two or more levels. In addition to comminuted fractures, they rank among the most severe fractures of the locomotor system. They most often occur under the influence of strong trauma in traffic and industrial trauma. Between the two levels of fracture on the tibia, there is an intermediate fragment, the part of the tibia that separates the two centres of fracture. The length of the intermediate fragment can vary from 3 to 20 centimetres (Figure 1). Figure 1. Segmental tibial fracture.
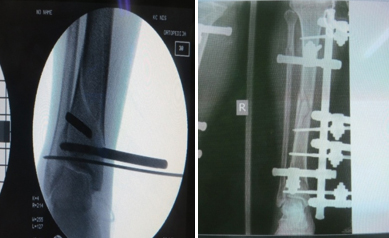
Comminution can be present in both fracture points [1,2,3]. THE AIM OF THE PAPERThe aim of this paper is to present the treatment of a female patient with a segmental tibial fracture, by using the method of external skeletal fixation. MATERIALS AND METHODSThe patient was treated at the Clinic for Orthopaedics and Traumatology of the Clinical Centre in Niš by using the method of external skeletal fixation, without opening the fracture point. After the operation, the patient was followed up for five years. CASE REPORTThe forty-year-old female patient suffered a severe closed segmental tibial fracture after falling from a height (Figures 2 and 3). Figures 2 and 3. Segmental tibial fracture, with two fracture points in the proximal and distal part of the tibia.
Right after admission, preoperative preparation was started and the patient was operated on; after repositioning under X-ray control, fracture stabilization was performed with two wedges in the proximal, two in the distal part of the tibia and two wedges in the intermediate fragment (Figures 4 and 5). Figures 4 and 5. Segmental fracture stabilized by external skeletal fixator "Mitković", after fracture repositioning under X-ray control
During hospital treatment, the patient had the wounds regularly dressed around the wedges of the external skeletal fixator and activated with the help of underarm crutches. (figure 6). Figure 6. Segmental tibial fracture stabilized by an external skeletal fixator.
After completing the hospital treatment, the patient was referred
to physical therapy in Ribarska Spa. After completing the
rehabilitation in the spa, the patient continued with the
rehabilitation in the place of living. The support on the operated
leg was gradually increased. Slowed fracture healing was registered
in both the proximal and distal fracture points. After the fracture
healed in both the proximal and distal part of the tibia, the
external skeletal fixator was removed. Figures 7 i 8. X-ray of the tibia five years after segmental fracture and external skeletal fixation.
Clinical examination revealed that there was no shortening of the injured leg, that there were no angular deformities and that the patient had a firm and stable support. (figures 9 and 10). Figures 9 and 10. The legs are of equal length, without angular deformities, which enables stable and firm support on the injured leg.
DISCUSSIONAccording to the data from the literature, the frequency of
segmental tibial fractures ranges from 1% do 6%. In over 60% of
cases, these are open tibial fractures. Segmental tibial fractures
are rarely an isolated injury, and they are frequently found in
polytraumatized patients [2,3]. CONCLUSIONSegmental tibial fractures belong to the group of the most severe fractures of the locomotor system. External skeletal fixation is one of the methods of treatment of both closed and open tibial fractures. If possible, X-ray-controlled fracture repositioning should be performed, without opening the point of the segmental fracture. If it is an open segmental fracture, it is necessary to perform primary treatment of the open fracture wound, external skeletal fixation, prescribe anti-tetanus protection and antibiotic therapy (Longacef and Amicacin, Metronidazole 500m/8h). In both closed and open segmental fractures, low molecular weight heparin (Fraxiparine) is prescribed to prevent thrombosis and pulmonary thromboembolism , and Forticolinn in order to stimulate fracture healing. LITERATURE:
|
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||