| |
|
|
INTRODUCTION
Alcohol consumption is increasingly a socially acceptable
activity, favored to the level of a mandatory ritual in many social
situations [1]. Globally, approximately 90% of people consume
alcohol at some point in their lives, while 3-5% is women and 10%
are addicted to alcohol[1]. Alcohol is a risk factor for 60
different medical conditions, and more than 4% of diseases are
directly related to alcohol consumption [2]. The economic burden of
alcohol consumption is estimated at more than 1% of the gross
national product in middle-developed and highly developed countries
[3]. Tolerance of the environment to alcohol consumption is high, so
from the intake of small doses of alcohol to clinical and physical
signs of intoxication, a lot of valuable time passes[4]. Society
enters the scene too late, usually with its system of condemnation
and isolation4. As a result, alcohol abuse causes approximately 3
million deaths each year (5.3% of deaths) [3].
Spirituality encompasses the existential need of each individual to
find answers and discover the purpose of life as well as the need to
believe in something greater than ourselves that connects all people
with each other [5,6]. Existential well-being implies a sense of the
meaning and purpose of existence, competence and the ability to
accept limitations [7]. Low levels of perceived meaning of one's own
life predispose to excessive alcohol consumption [8]. The content
and clarity of religious norms on alcohol use and the religiosity of
the individual determine the influence of religion on alcohol
consumption [9]. Christianity has prescribed norms on the use of
wine (not alcohol) in worship, but does not restrict moderate
consumption of alcohol (strong drinks), for refreshment or health
reasons [10]. The religiosity of the individual is a significant
modifier of the structure of values, as well as an important
predictor of a wide range of attitudes and behaviors, including
alcohol consumption4.
The aim of the research was to determine the frequency of alcohol
consumption and to assess the connection between the determined
consumption and the religiosity and existential well-being of the
adult population of the Orthodox religion in Krupa na Uni.
METHODS
The test as a cross-sectional study was conducted in a period of
three months, from 01.08.2021. to 11.01.2021. The respondents were
registered in the family medicine team of the Primary Health care
Center of the Krupa Health Center in Uni. During the regular work in
the family medicine Center, 103 adults aged 20 to 65 were selected
by random sampling. The study did not include people diagnosed with
alcoholism spectrum disorder or syndrome involved in treatment,
rehabilitation and resocialization, people with mental illness or
disorder, malignant and advanced chronic diseases. Data were
collected on the basis of anamnesis, available medical documentation
and filling out specific questionnaires.
The Alcohol Use Disorders Identification Test (AUDIT) was developed
and recommended by the World Health Organization for the early
identification of risky and harmful drinking as well as alcohol
dependence [11,12]. It consists of three questions in the field of
risky alcohol use (frequency of drinking, typical amount, frequency
of heavy drinking), four questions in the field of harmful alcohol
use (guilt after drinking, amnesia, injuries due to alcohol
consumption, environmental concerns) and three questions (decreased
control over drinking, increased desire to drink, morning drinking)
which are scored 0-4 [11,12]. The measuring range ranges from 0 (not
drinking) to 40 (alcohol abuse). A total score of 0 indicates
non-consumption of alcohol, 1-7 on low-risk drinking, 8-15 on risky
drinking and 20-40 on alcohol abuse [11,12]. The questionnaire has
acceptable internal reliability (Cronbach's alpha coefficient 0.86)
[13].
The Spiritual Well-Being Scale (SWBS) assesses two dimensions of
spiritual well-being, religiosity and existential well-being
[14,15]. The Religious Well-Being subscale (RWB) evaluates the
relationship with God, while the Existential Welfare subscale (EWB)
analyses the sense of meaning and purpose of existence, competence
and ability to accept limitations [14,15. The subscales contain ten
questions with answers on the Likert scale of 6 points ranging from
"strongly agree" (1) to "strongly disagree" (6) [14,15]. Eight
questions were written in the reverse direction and the reverse was
scored [14,15]. The measuring range of the questionnaire ranges from
20 to 120, the measuring range of the subscale from 10 to 60
[14,15]. The overall questionnaire score of 20 to 40 indicates low,
41 to 99 moderate, and 100 to 120 high spiritual well-being [14,15].
The total result of the subscale from 10 to 20 is interpreted as
low, from 21 to 49 as moderate and from 50 to 60 as high religiosity
or existential well-being [14,15]. The subscales have acceptable
internal reliability (Cronbach’s alpha coefficients 0.91 and 0.84)
[14,15]. For specific purposes, e.g. focusing only on religiosity
and / or only on existential well-being, the authors allow
individual use of subscales [14].
Contingency tables based on the nonparametric Chi square test were
used to determine statistical significance. The significance level
is set to 95% confidence interval. The results are presented
textually and tabular, the complete work is processed in the text of
the Microsoft Word processor for Windows. P values that could not be
expressed to a maximum of three decimal places are shown as p <0.001
[16].
RESULTS
The study included 103 adults aged 20 to 65 years. Among them were
57 (55.3%) men and 46 (44.7%) women. The mean age of the examined
population was 44.7 ± 10.45 years.
Alcohol was not consumed by 21 (20.4%) participants in the study,
while 82 (79.6%) consumed it with different frequency (low-risk
drinking 53.4%, risky drinking 16.5%, harmful drinking 2.9% and
alcohol abuse 6.8%).
Risky drinking was found in 15 (14.6%) men, harmful drinking in 3
(2.9%) and alcohol abuse in 6 of them (5.8%). Harmful drinking was
not found in women, 2 (1.9%) women drank at risk and 1 (1%) abused
alcohol. Males were significantly more likely to consume alcohol (p
<0.0001). Table 1.
Table 1: . Interrelations between a participants' gender and alcohol
drinking forms according to the Alcohol Use Disorders Identification
Test score

*AUDIT score 0; **AUDIT score 1-7; ***AUDIT score 8-15; ****
AUDIT score 16-19; ***** AUDIT score 20-40; 1p according to Chi
Quadrat Test.
Out of a total of 16 (15.5%) respondents aged 20 to 34, none abused
alcohol, while only 1 (1%) consumed alcohol within the limits of
harmful drinking. Out of a total of 49 (47.6%) respondents aged 35
to 49, none consumed alcohol within the limits of harmful drinking,
while 3 (2.9%) abused alcohol. Of the remaining 38 (36.9%)
respondents aged 50 to 65, 2 (1.9%) consumed alcohol within the
limits of harmful drinking, while 4 (3.9%) abused alcohol. Age did
not have a significant effect on alcohol consumption (p = 0.587).
Table 2.
Table 2. Interrelations between a participants' age structure and
alcohol drinking forms according to the Alcohol Use Disorders
Identification Test score
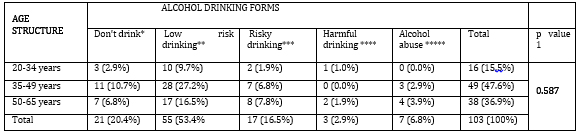
*AUDIT score 0; **AUDIT score 1-7; ***AUDIT score 8-15; ****
AUDIT score 16-19; ***** AUDIT score 20-40; 1p according to Chi
Quadrat Test.
Low religiosity was found in 3 (2.9%) respondents, moderate in 70
(68.0%), while 30 (29.1%) were highly religious. The average value
of the subscale of religiosity of the respondents was 41.75
(moderate religiosity) with an average deviation of 10.23. In the
group of low-religious respondents, there were no respondents who do
not drink and consume alcohol within the limits of low-risk
drinking. On the other hand, in the group of highly religious
respondents, there were no respondents who drink or abuse alcohol. A
significant correlation/influence of religiosity on alcohol
consumption was found among the respondents (p <0.0001). Table 3.
Table 3: Interrelations between a participants' religiosity
according to po Religious Well-Being score and alcohol drinking
forms according to the Alcohol Use Disorders Identification Test
score
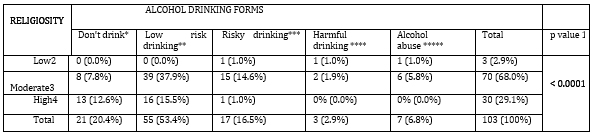
*AUDIT score 0; **AUDIT score 1-7; ***AUDIT score 8-15; **** AUDIT
score 16-19; ***** AUDIT score 20-40; 1p according to Chi Quadrat
Test. ; RBW score 10-20; 3RBW score 21-49; 4RBW score 50-60.
Low existential well-being was found in 8 (7.8%) respondents,
moderate in 70 (68.0%) and high existential well-being in 25
(24.2%). The average value of the subscale of existential well-being
of the respondents was 40.36 (moderate existential well-being) with
an average deviation of 10.93. In the group of respondents with low
existential well-being, the largest number of respondents abuse
alcohol, 5 (4.9%). There were no respondents who do not drink and
consume alcohol within the limits of low-risk drinking. On the other
hand, in the groups with high existential well-being, there were no
respondents who consume alcohol within the limits of risky drinking,
drink harmful or abuse alcohol. A significant correlation/impact of
existential well-being on alcohol consumption was found in the
subjects (p <0.0001). Table 4.
Table 4: Interrelations between a participants' existential
well-being according to po Existential Well- Being score and alcohol
drinking forms according to the Alcohol Use Disorders Identification
Test score
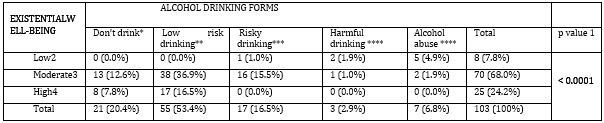
*AUDIT score 0; **AUDIT score 1-7; ***AUDIT score 8-15; ****
AUDIT score 16-19; ***** AUDIT score 20-40; 1p according to Chi
Quadrat Test. ; EBW score 10-20; 3EBW score 21-49; 4EBW score 50-60.
DISCUSSION
Excessive alcohol consumption impairs the physical and mental health
of the consumer and adversely affects the health and well-being of
persons in his environment17. Worldwide, 32.5% of people consume
alcohol (25% of women and 39% of men) [17]. The average amount of
alcohol consumed is 0.73 standard drinks per day for women and 1.7
standard drinks per day for men17. A small but significant part
(3.5% in developed countries) of the adult population has developed
alcohol dependence, while risky and harmful drinking has been
identified in a significantly higher percentage (15-40%) [18].
The average daily intake of pure alcohol in Bosnia and Herzegovina
is 29 g (13.4 l of pure alcohol, of which 75.8% beer, 8.6% wine,
12.4% spirits and 3.2% other alcoholic beverages) [19]. Alcohol
intoxications were recorded in 22.7% of the population (36.4% of men
and 8.6% of women) [19]. Harmful drinking was found in 2.5% of the
population, alcohol dependence at 3.4%. Approximately 19.6.0% of the
population has health problems due to alcohol use [19]. Alcohol use
is the cause of death in 4.6% of the population of Bosnia and
Herzegovina (7.7% of men and 1.5% of women) [19].
In our study, 79.6% of respondents consumed alcohol (53.4% low-risk
drinking, 16.5% risky drinking, 2.9% harmful drinking and 6.8%
alcohol abuse). Males were more likely to consume alcohol. The age
of the respondents did not have a significant impact on alcohol
consumption.
Religiosity encompasses five fundamental dimensions inherent in all
religions: ideological (expectation that a religious person will
accept certain beliefs), experiential (expectation that a religious
person will experience religious feelings), ritual (encompasses
specific religious practices required of a religious person),
intellectual (expectation that the religious person will be
acquainted with the basic principles of his faith), consequential
(includes the secular effects of religious belief, practice and
experience on the religious person) [4,20].
Religiosity is a significant modifier of the structure of values, as
well as an important predictor of a wide range of behaviors and
attitudes [21,22]. It allows moral values to receive a supernatural
sanction that empowers them in their obligation and coercion
[21,22]. It contributes to the respect of authority and institutions
in general, because God, especially monotheistic, is a symbol of
social authority [21,22]. It has a positive effect on self-control
and resistance to negative influences [21,22]. It can answer the
question of the meaning and value of life which can consequently
reduce the attractiveness of alcohol consumption [21,22].
The protective influence of religiosity on alcohol consumption is
also determined by the specificity of religion [10]. It is assumed
that members of religious groups that are characterized by strict
and clear prohibitions on alcohol consumption will resort to it to a
lesser extent [10].
Islam completely forbids the production, sale, donation and keeping
of alcohol in the homes of believers [10]. On the other hand,
Christianity does not have completely clear guidelines or
restrictions regarding the quantity or purpose of the use of alcohol
outside religious ceremonies (consumption of alcohol for refreshment
or health reasons is allowed) [11].
All participants in the research were of the Orthodox faith.
Moderate religiosity was found in 68% of respondents, high in 29%
and low in 3%. The religiosity of the respondents had a significant
impact on alcohol consumption (p <0.001).
A 38-year prospective cohort study involving 1,795 children of
Hindu, Islamic and Christian faiths from the island of Mauritius
found that religious affiliation reduces the likelihood of drinking
by adults who believe their religion promotes abstinence [10]. A
survey of 526 third- and fourth-year students at eight faculties of
the University of Tuzla found a strong association between all 5
domains of religious status and patterns of alcohol consumption4. A
survey of 495 adults (Christians, Muslims, Buddhists, and
nonreligious adults) in the United States found that nonreligious
adults and Buddhists had significant positive attitudes toward
alcohol use toward Christians and Muslims [23]. A study in Scotland
involving 4,066 students found that non-religious students consumed
significantly more alcohol (women more than 14 standard drinks per
week, men more than 21 standard drinks per week) [24]. A study in
Yemen among 146 adults in two centers for the treatment of alcohol
and other psychoactive substance addiction found that religiosity
plays an important role in the process of recovery and prevention of
re-abuse [25]. A survey in Brazil among 3,007 adults in 143 cities
identified a strong association between religiosity and negative
attitudes toward alcohol, including limited sales time, reduced
store availability, ban on advertising, tax increases, and minimum
legal benefits for alcohol consumption [26].
Existential well-being is determined by the essential issues of
human existence and the ability to engage in the process of creating
meaning [27]. Meaning does not come from human existence itself, it
is something that an adult faces and discovers[28]. Taking
existential responsibility for one's life (accepting or rejecting
the offered meaning) each individual comes to the consciousness of
the same self [28].
The absence of meaningfulness (existential vacuum) reduces the
perception of the meaning of one's own life and predisposes to
potentially risky behaviors29. In addition, it causes apathy,
emptiness, low self-esteem and frustration [28,29].
By consuming alcohol, an existentially frustrated adult creates the
illusion of meaning, belonging and self-esteem [27].
68% of respondents had moderate existential well-being, 24.2% high
and 7.8% low. The existential well-being of the respondents had a
strong influence on alcohol consumption (p <0.001)
A study of 151 students aged 18 to 25 in the United States
identified an inverse association of existential well-being with
patterns of alcohol consumption and the likelihood of attending a
social event that included alcohol [30]. In addition, existential
well-being is an important predictor of alcohol prevention [30]. A
study of 176 adults aged 18 to 30 in Australia found significantly
higher alcohol consumption in the presence of an existential vacuum
[29]. A study in Canada, which included 131 adults hospitalized in a
psychiatric clinic, found that an addiction treatment program
contributes to the growth of meaningful life [31].
CONCLUSION
Almost 80% of the participants in the research consumed alcohol, of
which two-thirds were part of low-risk drinking. Males were
significantly more likely to consume alcohol. The age of the
respondents did not have a significant impact on alcohol
consumption.
All respondents are of the Orthodox faith. Most are moderately
religious. There is a significant correlation/influence of
religiosity in alcohol consumption among respondents.
Most study participants have a moderate degree of existential
well-being. Participants with a high degree of existential
well-being consume significantly less alcohol, compared to
respondents who have moderate or low existential well-being.
LITERATURE:
- Sher L. Depression and alcoholism. QJM: An International
Journal of Medicine. 2004; 97(4):237–240. Available from:
https://academic.oup.com/qjmed/article/97/4/237/1525431
- Žuškin E, Jukić V , Lipozenčić J, Matošić A, Mustajbegović
J, Turčić N et al. Alcohol and workplace. Arh Hig Rada Toksikol.
2006;57:413-426. Available from:
https://hrcak.srce.hr/file/9214.
- Glantz MD, Bharat C, Degenhardt L, Sampson NA, Scott KM, Lim
CCW et al. WHO World Mental Health Survey Collaborators. The
epidemiology of alcohol use disorders cross-nationally: Findings
from the World Mental Health Surveys. Addict Behav.
2020;102:106128. Available from:
https://psycnet.apa.org/record/2020-24294-001
- Jašić O, Hodžić Dž, Selmanović S. Utjecaj religijskog
statusa i kvalitete života na konzumaciju alkohola među
studentskom populacijom Sveučilišta u Tuzli. JAHR. 2012;3(5).
Available from: https://hrcak.srce.hr/file/130059.
- Leutar Z, Leutar I. Religioznost i Duhovnost u socijalnom
radu. Crkva u svijetu. 2010;45(1):78-103. Available from:
https://hrcak.srce.hr/file/76620
- Dučkić A, Blažeka Kokorić S. Duhovnost – resurs za
prevladavanje kriznih životnih situacija kod pripadnika
karizmatskih zajednica. Ljetopis socijalnog rada.
2014;21(3).425-452. Available from:
https://www.academia.edu/49511095/Duhovnost_Resurs_Za_Prevladavanje_Kriznih_%C5%BDivotnih_Situacija_Kod_Pripadnika_Karizmatskih_Zajednica
- Visser A, Garssen B, Vingerhoets AJJM. Existential
Well-Being Spirituality or Well-Being? The Journal of Nervous
and Mental Disease. 2017;205(3),234-241. Available from:
https://journals.lww.com/jonmd/Abstract/2017/03000/Existential_Well_Being_
Spirituality_or.13.aspx
- Vondras DD, Schmitt RR, Marx. Associations between aspects
of spiritual well-being, alcohol use, and related
social-cognitions in female college students. Journal of
Religion and Health. 2007;46(4):500-515- Available from:
https://www.jstor.org/stable/27513039
- Luczak SE, Prescott CA, Dalais C, Raine A, Venables PH,
Mednick SA. Religious factors associated with alcohol
involvement: results from the Mauritian Joint Child Health
Project. Drug Alcohol Depend 2014;135:37-44. Available from:
https://www.researchgate.net/publication/259317859_Religious_Factors_Associated_
with_Alcohol_Involvement_Results_from_the_Mauritian_Joint_Child_Health_Project
- Golik-Gruber V. Alkohol u očima vjerskih zajednica. U:
Zbornik stručnih radova Alkohološkog glasnika. Zagreb
2003;74-76. Available from:
http://www.moravek.org/kla/61-003.html.
- Toković S, Bivolarević S, Đurišić Lj, Arsić A, Čeković J,
Srećkov M et al. Alkoholizam i psihijatrijski komorbiditet u
primarnoj zdravstvenoj zaštiti. Sanamed. 2010;5:35-38. Available
from:
http://www.sanamed.rs/sanamed_pdf/sanamed_5/Snjezana_Tokovic.pdf
- Skandul D, Ožvačić Adžić Z, Hanževački M, Šimić D. Procjena
poremećaja uzrokovanih alkoholom u radu obiteljskog liječnika-pilot
istraživanje. Procjena poremećaja uzrokovanih alkoholom u radu
obiteljskog liječnika – pilot istraživanje Med Fam Croat.
2017;25(1-2):17-16. Available from:
https://hrcak.srce.hr/file/277174
- Rubio Valladolid G, Bermejo Vicedo J, Caballero Sánchez-Serrano
MC, Santo-Domingo Carrasco J. Validación de la prueba para la
identificación de trastornos por uso de alcohol (AUDIT) en
Atención Primaria [Validation of the Alcohol Use Disorders
Identification Test (AUDIT) in primary care]. Rev Clin Esp.
1998;198(1):11-4. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7676097
- Malinakova K, Kopcakova J, Kolarcik P, Geckova AM, Solcova
IP, Husek V et al. The Spiritual Well-Being Scale: Psychometric
Evaluation of the Shortened Version in Czech Adolescents. J
Relig Health. 2017;56(2):697-705. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5320003/
- Nakane S. The Influence of Faith and Religiosity in Coping
with Breast Cancer. ARC Journal of Psychiatry. 2017; 2(4): 1-8.
Available from:
https://www.arcjournals.org/journal-of-psychiatry/volume-2-issue-4/1.
- Petrovečki M. Statistički temelji znanstvenoistraživačkog
rada, u: Matko Marušić (ur.), Uvod u znanstveni rad u medicini.
Medicinska Naklada. Zagreb. 2000.
- Griswold MG, Fullman N, Hawley C, Arian N, Zimsen SRM,
Tymeson HD et al. Alcohol use and burden for 195 countries and
territories, 1990–2016: a systematic analysis for the Global
Burden of Disease Study. 2016. Lancet 2018; 392:1015–35.
Available from:
https://www.thelancet.com/article/S0140-6736(18)31310-2/fulltext
- Babor TF, Higgins-Biddle JC. Brief Intervention For
Hazardous and Harmful Drinking. A Manual for Use in Primary
Care. 2001. Available from:
https://www.drugsandalcohol.ie/14105/1/WHO_Brief_intervention.pdf.
- Geneva: World Healh Organization. Global status report on
alcohol and health 2018. Geneva: World Health Organization.
2018. Available from:
https://www.who.int/publications/i/item/9789241565639.
- Jusić M. Psihološka dimenzija religije i religijske
motivacije. Novi muallim. 2006;25(29):60-65. Available from:
https://www.ceeol.com/search/article-detail?id=568406.
- Flere S. Religioznost i delikventnost: istraživačke
rezultati na populaciji mariborskih studenata. Druš. Istraž.
Zagreb 2005;3(77):531-544. Available from:
https://hrcak.srce.hr/17856.
- Rohrbaugh J, Jessor R. Religiosity in youth: A personal
control against deviant behavior. Journal of personality. 1975;
43(1):136-155. Available from:
https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1467-6494.1975.tb00577.x?sid=nlm%3Apubmed
- Najjar LZ, Leasure L, Henderson CE, Young CM, Neighbors C.
Religious perceptions of alcohol consumption and drinking
behaviours among religious and non-religious individuals. Mental
Health Religion & Culture. 2017;19(9):1-14. Available from:
https://www.tandfonline.com/doi/abs/10.1080/13674676.2017.1312321?journalCode=cmhr20
- Engs RC, Mullen K. The Effect of Religion and Religiosity on
Drug Use Among a Selected Sample of Post-Secondary Students in
Scotland. Addiction Research. 1999;7(2):149-170. Available from:
https://www.tandfonline.com/doi/abs/10.3109/16066359909004380
- Al-Omari H, Hamed R, Abu Tariah H. The Role of Religion in
the Recovery from Alcohol and Substance Abuse Among Jordanian
Adults. J Relig Health. 2015;54(4):1268-77. Available from:
https://www.researchgate.net/publication/262024828_The_Role_of_Religion_in_the_Recovery_
from_Alcohol_and_Substance_Abuse_Among_Jordanian_Adults
- Lucchetti G, Koenig HG, Pinsky I, Laranjeira R, Vallada H.
Religious beliefs and alcohol control policies: a Brazilian
nationwide study. Rev. Bras. Psiquiatr. 2014;36(1). Available
from:
https://www.scielo.br/j/rbp/a/qQvmCC4HpwhQFvGpKLZvPjR/?lang=en
- Sung L. An Exploration of Existential Group Art Therapy for
Substance Abuse Clients with a History of Trauma. LMU/ LLS
Theses and Dissertations. 2016. Available from:
https://digitalcommons.lmu.edu/cgi/viewcontent.cgi?article=1285&context=etd
- Radinov T. Smisao života i patnje promatran kroz katoličko–teološku
i psihološko–logoterapijsku perspektivu. Obnov život.
2017;72(4):517–529. Available from: https://hrcak.srce.hr/193039
- Csabonyi M, Phillips LJ. Meaning in Life and Substance Use.
Journal of Humanistic Psychology. 2020;60(1):3-19. Available
from:
https://journals.sagepub.com/doi/full/10.1177/0022167816687674
- Wood RJ, Hebert EP. The relationship between spiritual
meaning and purpose and drug and alcohol use among college
students. American Journal of Health Studies.
2005;20(1/2):72-79. Available from:
https://www.researchgate.net/publication/235349772_The_relationship_between_
spiritual_meaning_and_purpose_and_drug_and_alcohol_use_among_college_students
- Waisberg JL, Porter JE. Purpose in life and outcome of
treatment for alcohol dependence. Br J Clin Psychol.
1994;33(1):49-63. Available from: https://bpspsychub.onlinelibrary.wiley.com/doi/abs/10.1111/j.2044-8260.1994.tb01093.x?sid=nlm%3Apubmed
|
|
|
|