|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
Original papers IMPACT AND ASSESSMENT OF NUTRITIONAL STATUS IN PATIENTS UNDERGOING TREATMENT FOR COLORECTAL CANCER Teodora Filipović (1,4), Dalibor Perić (2,4), Natalija Jovanović (3,4) (1) DOM OF HEALTH KUČEVO; (2) GNJILANA HEALTH CENTER; (3) DOM OF HEALTH IN NIŠ; (4) FACULTY OF MEDICINE OF THE UNIVERSITY OF NIS |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Download in pdf format | Summary:
Introduction: Hypertension is one of the most significant risk
factors for cardiovascular diseases and a leading cause of morbidity
and mortality worldwide. During the COVID-19 pandemic, an increase
in the number of individuals with newly diagnosed hypertension was
observed, suggesting a possible association between SARS-CoV-2
infection, immune response, and vascular changes. Aim: To
examine a possible association between COVID-19 infection,
SARS-CoV-2 vaccination, and the occurrence of hypertension in the
adult population. Materials and Methods: The study was
conducted using an anonymous questionnaire that included 203
respondents of both sexes and three age categories. Lifestyle
factors, previous COVID-19 infection, vaccination status, and the
occurrence of hypertension were descriptively analyzed. Results:
Of the total 203 respondents, 72.9% were female and 27.1% male. A
total of 144 respondents (70.9%) had a history of COVID-19
infection, and 43 individuals (21.2%) had diagnosed hypertension.
Among them, 17 individuals (40.5%) initiated antihypertensive
therapy within the last 5 years, following COVID-19 infection. A
total of 59.1% of respondents were vaccinated, and the majority did
not report adverse effects. Conclusion: The results indicate
a statistically significant association between COVID-19 infection
and increased incidence of hypertension in the post-pandemic period
(χ² = 21.3; p < 0.001), while vaccination against COVID-19 was not
statistically significantly associated with newly developed
hypertension.. Keywords: COVID-19, hypertension, vaccination, SARS-CoV-2, cardiovascular risk. |
|||||||||||||||||||||||||||||||||||
|
INTRODUCTION Hypertension (HTN) is the most common chronic
disease of modern society and a leading risk factor for the
development of coronary artery disease, cerebrovascular events, and
chronic kidney disease [1]. The global COVID-19 pandemic, caused by
the SARS-CoV-2 virus, has prompted numerous studies on the impact of
infection on the cardiovascular system. Proposed mechanisms include
inflammatory processes, endothelial dysfunction, and dysregulation
of the renin–angiotensin–aldosterone system (RAAS). [2,3]. AIM The aim of this study was to analyze the potential association between COVID-19 infection, SARS-CoV-2 vaccination, and the occurrence of hypertension in adults, while also assessing additional risk factors (sex, age, smoking, physical activity, and diet). MATERIAL AND METHODS The study was conducted during 2025 on a sample of 203
participants. The questionnaire consisted of 25 questions covering
sociodemographic characteristics, dietary habits, physical activity,
smoking, alcohol consumption, as well as data related to COVID-19
infection and vaccination. The analysis was performed descriptively
using percentage distributions and hypothesis testing. Special
emphasis was placed on participants with hypertension, the date of
initiation of therapy, and a possible association with previous
COVID-19 infection. The data were processed descriptively and
analytically using SPSS v.26 software. Statistical significance
testing was performed using the chi-square (χ²) test for categorical
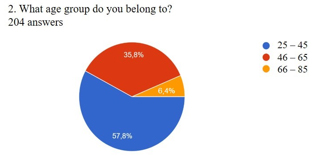
variables. Statistical significance was accepted at p < 0.05.. RESULTS Age structure of participants (Figure 1): Out of 203 respondents, the most represented group was the younger population aged 25–45 years (57.6%), followed by the middle-aged group of 46–65 years (35.8%), while the older population aged 66–85 years was the least represented (6.4%). Graph 1. Distribution of the age structure of respondents
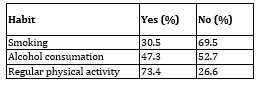
Gender structure and hypertension: Table 1. Habits and risk factors
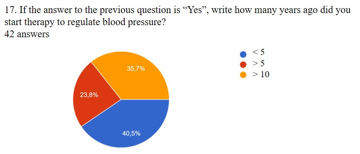
Diet and anthropometric data: Chart 2. Distribution of respondents as a function of time of initiation of therapy for blood pressure regulation
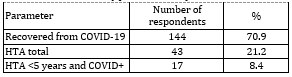
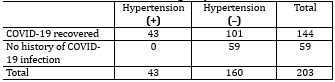
COVID-19 infection and hypertension: A total of 144 participants
(70.9%) had previously had COVID-19 infection, while only 13 (9.0%)
experienced a more severe form of the disease. Hospitalization was
reported in only 4 participants. Table 2. Association between COVID-19 infection and hypertension (HTA)
A statistically significant association between previous COVID-19 infection and the presence of hypertension was analyzed using the χ² test: the relationship between COVID-19 infection and the occurrence of hypertension. The contingency table (COVID +/− × HTA +/−) showed a significant correlation: χ² = 21.3; df = 1; p < 0.001, indicating that individuals who had previously had COVID-19 were significantly more likely to develop new-onset hypertension and initiate treatment after the pandemic compared to those who were not infected (Table 3). Table 3. Contingency table
(This includes the 17 newly diagnosed cases after COVID-19 infection, as all HTA+ participants are included in this row) There is a statistically significant association between COVID-19
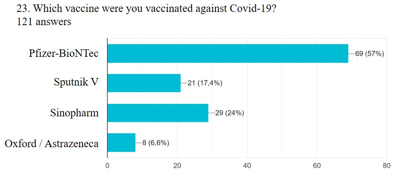
infection and newly diagnosed hypertension (p < 0.001). Figure 3. Graphical representation of the distribution of administered COVID-19 vaccines by manufact
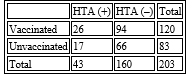
Table 4. Contingency table (derived from text)
(The distribution was estimated based on proportions; no difference in the frequency of adverse effects was observed.) Gender and age could not be analyzed numerically. DISCUSSION Results indicate that there is a statistically significant association between previous COVID-19 infection and the occurrence of hypertension, particularly new-onset arterial hypertension (defined as hypertension diagnosed within less than 5 years). These findings are consistent with other studies suggesting that the SARS-CoV-2 virus affects ACE2 receptors, leading to endothelial dysfunction and increased blood pressure [13,14]. Notably, 40.5% of hypertensive patients initiated therapy after the pandemic, which is statistically significant and may indicate post-COVID hypertension. Most participants in the newly developed post-COVID hypertension group had a mild form of the disease, suggesting that even subclinical damage may have long-term consequences [15]. According to the survey data, vaccination did not have a statistically significant impact on the occurrence of hypertension—most vaccinated participants did not report adverse effects, nor was an increase in blood pressure observed following immunization. This is consistent with published meta-analyses showing that COVID-19 vaccines do not increase the risk of hypertension [16,17]. The results of this study indicate a clear trend toward increased incidence of newly diagnosed hypertension in the post-COVID period. The fact that 40% of hypertensive participants initiated therapy within the last five years, all of whom had a history of COVID-19 infection, supports the hypothesis of a possible pathophysiological link between SARS-CoV-2 and long-term vascular changes. This finding aligns with an increasing body of evidence suggesting that infection may induce persistent alterations in blood pressure regulation, including endothelial inflammation, ACE2 receptor disruption, RAAS activation, increased arterial stiffness, and autonomic dysfunction. Such findings support the concept of “silent endothelial injury,” where viral infection causes subclinical damage that becomes clinically evident over time. Additionally, studies indicate that post-COVID syndrome may include autonomic dysregulation, characterized by blood pressure variability, palpitations, and tachycardia, which may also contribute to the development of hypertension. Regarding vaccination, our data suggest that no significant increase in hypertension was observed following immunization in the studied population. This is consistent with the majority of published meta-analyses showing that episodes of elevated blood pressure after vaccination are most often transient, mild, and without long-term consequences. It is also important to emphasize the significant influence of lifestyle and anthropometric factors. In our sample, obesity was relatively common, while physical activity was present in most participants but often only of moderate intensity. These parameters, along with a positive family history, are well-known risk factors for hypertension and may partially explain the increased prevalence, particularly during periods of reduced physical activity and increased stress during the pandemic. When all factors are considered together, it may be assumed that in many individuals a combined effect of infection, stress, altered lifestyle habits, and pre-existing predisposition contributed to the manifestation of hypertension. The findings of this study complement existing literature and highlight the need for further multidisciplinary approaches, including cardiological, endocrinological, and immunological perspectives. CONCLUSION The results of this study confirm that there is a statistically
significant association between previous COVID-19 infection and an
increased incidence of newly diagnosed hypertension in the
post-pandemic period. In a substantial number of participants,
hypertension developed after 2020, which temporally corresponds to
the pandemic and supports findings from international studies on the
long-term cardiovascular consequences of SARS-CoV-2 infection.
According to our results, vaccination does not play a role in the
development of hypertension. These findings are consistent with
current evidence indicating that the risk of hypertension associated
with vaccination is low and most often transient. In the context of
risk factors, the presence of obesity, a positive family history,
and unhealthy lifestyle habits such as smoking and increased alcohol
consumption, as is well established, may further contribute to the
development of hypertension. Overall, the data suggest that COVID-19
infection is a significant health event that, in predisposed
individuals, may accelerate or precipitate the onset of
hypertension. Further, larger-scale and longitudinal studies are
necessary to more precisely define the relationships between viral
infection, immune response, vascular regulation, and long-term
cardiovascular outcomes. LITERATURE: 1. WHO. Hypertension fact sheet. World Health Organization; 2023. Author contributions: Concept and design: Teodora Filipović and Dalibor Perić. Data collection: Teodora Filipović and Dalibor Perić. Statistical analysis: Dalibor Perić. Data interpretation: Teodora Filipović. Drafting of the manuscript: Teodora Filipović. Critical revision and final approval of the manuscript: Teodora Filipović, Dalibor Perić, and Natalija Jovanović. |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||