| |
|
|
INTRODUCTION Burnout syndrome, or burnout syndrome in
Anglo-Saxon literature, is a phenomenon in modern medicine that was
described in the seventies of the twentieth century. It was first
introduced into medical use by Freudenberger [1], and then
elaborated by Maslach et al. [2, 3]. It is the chronic stress
associated with an emotionally draining job that a person cannot
cope with with their self-help resources, resulting in burnout. The
syndrome is always associated with work, and in addition to
emotional exhaustion, it also implies depersonalization and the
impression of insufficient efficiency. There are many works on this
topic. It is described by professions.
Doctors feel exhausted with the impression of being used up at the
end of the shift and that they cannot provide the same quality
service to patients. The depersonalization of doctors means that
they view patients as an object, not as a human being, and they
become increasingly unkind. This is especially reflected in the
inability to help patients with their problems as well as in health
care. The professional progress of doctors also suffers [4,5,6,7].
"Managerial disease" is a term that can be synonymous with burnout,
and represents a set of symptoms that arise as a result of long-term
exposure to stress at work. Although the profession of
director-manager is associated with great responsibility and duties,
work overload leads to physiological and later psychosomatic
reactions. Deterioration of the health condition is accompanied by
extreme physical and psychological exhaustion [8,9,10].
Cause of burnout
The causes of burnout syndrome are: -imbalance between the
individual's personal psychological strengths and unfavorable
conditions at work: lack of autonomy in the workplace and work
control; work that conflicts with ethical and personal feelings;
lack of praise or support from the team or superiors; to strive even
though the goals are not what the individual deeply desires[11].
Dullness towards professions
Burnout syndrome among general practitioners is an increasingly
common phenomenon with serious consequences for professional
efficiency, the quality of health care, and the personal mental
health of health workers. Doctors often feel emotional isolation,
overwhelm and loss of meaning in their work.
Nurses are also a work load. Nurses in intensive care or who work at
an oncology clinic are particularly exposed to this syndrome [12].
Managers, directors, and especially employees in banking have been a
frequently studied occupational group in the literature. In recent
years, numerous studies have also been published on burnout among
employees in the telecommunications sector. These jobs are highly
exhausting, as the performance targets that employees must achieve
on the one hand, and very limited interpersonal interaction among
employees on the other, create a favorable environment for the
development of burnout syndrome. These are sedentary jobs with very
little physical activity. It is considered that this profession
involves all three dimensions of burnout: job demands, lack of
adequate managerial control, and reduced interaction among employees
[13, 14].
Clinical picture
Stress is experienced and processed differently by each
individual, so symptomatology also varies.
Symptoms of burnout include mental and psychological fatigue,
reduced immune response leading to more frequent illness, recurrent
headaches, back pain, muscle pain, feelings of fear when going to
work, anger and irritability, as well as feelings of helplessness,
failure, hopelessness, and loneliness. Individuals often require
more time to complete assigned tasks.
All professions with high levels of responsibility and workload, in
which physiological and later psychosomatic reactions occur due to
overload, may lead to deterioration of health status and eventual
physical and mental exhaustion. The most common manifestations
include tachycardia, palpitations, excessive sweating, elevated
blood glucose levels, increased cholesterol, and elevated blood
pressure. The so-called “managerial disease” can be considered an
epidemic of the modern era, increasingly affecting people of younger
and middle age. The condition more frequently affects men than
women. In men, it most commonly leads to cardiac problems, while
women more often suffer from anxiety, apathy, and depression.
If acute health problems and symptoms are not treated adequately and
in time, they may become chronic. This is a syndrome of chronic
occupational stress, manifested as emotional exhaustion,
depersonalization, and a reduced sense of personal accomplishment
[15].
Among general practitioners, the incidence of this syndrome is
increasing due to excessive workload during the working day,
including scheduled and unscheduled patients, as well as detailed
documentation of each visit. Workload, rigid organizational
structure, a work policy that penalizes mistakes but does not reward
success, along with lack of personal resources, all contribute to
burnout syndrome.
Emotional support is often lacking. Burnout should be viewed as a
systemic warning signal that exhausts the employee, rather than a
personal weakness. Burnout is not merely job dissatisfaction or
fatigue due to workload; it manifests as a combination of stress and
depressive symptoms [16]. However, in some cases, these symptoms may
be absent.
Burnout has been described as closely related to depression, but the
presence of depersonalization and reduced professional achievement
clearly distinguishes it from depression and other psychiatric
conditions.
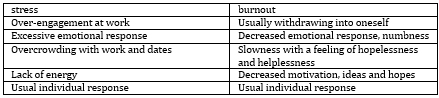
Consequences include reduced empathy, impaired patient
relationships, and deterioration of both physical and mental health
[17,18]. Table 1 presents the difference between stress and burnout.
Table 1. Difference between stress and burnout
Diagnosis of burnout syndrome
As many as 75–90% of all medical visits are related to chronic
stress, and patients often consult multiple available specialists in
order to reach a definitive diagnosis.
First, a detailed medical history is required, followed by a
physical examination and available laboratory tests to exclude other
clinical conditions. Burnout syndrome may also present with cardiac
symptoms, neurological manifestations, or psychiatric disorders
[19].
Principles of therapy
The principles of treatment are based on managing the symptoms and
signs of occupational burnout. Depending on which symptoms are
predominant, greater attention is given to their treatment.
In developed centers such as the Healthcare System, employees have
access to art therapy, music therapy, and mindfulness training
sessions through counseling services [20].
Role of psychiatrists and psychotherapists in patient care
Literature data indicate that some hospitals offer free mental
health support and counseling services for their employees.
Psychotherapy should not be an instrument for adapting individuals
to an exhausting system, but rather a means of preserving humanity,
empathy, and professional ethics. Individuals experiencing burnout
may sometimes hesitate to seek help and instead sink deeper into the
condition.
A study conducted in Singapore reported a donation-funded program
providing support to individuals facing various problems such as
work-related stress, relationship issues, and personal or family
dilemmas [21].
Preventive measures
Today, awareness of the importance of prevention is growing, and
employers increasingly recognize the value of investing in employee
health. Many encourage regular medical check-ups and provide
voluntary health insurance for workers. Regular systematic
examinations are an important preventive measure.
Preventive strategies include promoting a supportive workplace
culture, psychological support, workload rationalization, and
teamwork.
Common preventive measures include regular physical activity (as it
stimulates endorphin release), a well-balanced diet rich in fruits
and vegetables, boiled meat and fish rich in omega-3 fatty acids,
and regular sleep (to allow body recovery), as well as avoiding
harmful habits such as smoking, excessive alcohol consumption, and
caffeine intake. It is important to be aware of one’s own emotions
and strengthen self-confidence in order to recognize early signs of
burnout before they become severe. Finding meaning and satisfaction
in the work environment is also important. Flexible working hours
may also be considered.
A meta-analysis by Williams et al. indicated that physicians may
benefit from stress-reduction interventions, including changes in
organizational strategies, as the root of burnout lies in the
balance between work environment and private life [22].
Conclusion
This paper presents the etiological factors contributing to
burnout syndrome and highlights the characteristics of its clinical
presentation to facilitate disease recognition, as well as the
principles of treatment. The importance of psychotherapeutic support
in patient education and care is emphasized.
Burnout should be viewed as a systemic warning signal, and more
flexible working hours for employees should be considered.
Strategies for improving work–life balance should be further
developed. Interdisciplinary collaboration represents a key step
toward a healthier and more humane working environment and society
as a whole.
Literature:
1. Freudenberger HJ. Staff burnout. J Soc Issues 1974; 30:159–65.
2. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory
Manual, 3rd ed. Palo Alto, CA: Consulting Psychologists Press, 1996.
3. Schaufeli WB, Leiter MP, Maslach C. Burnout: 35 years of research
and practice. Career Dev Int 2009; 14: 204–20.
4. Schaufeli W, Bakker A, Hoogduin K, Schaap C, Kladler A. On the
clinical validity of the Maslach burnout inventory and the burnout
measure. Psychol Health 2001; 16: 565–82.
5. Bianchi R, Schonfeld IS, Laurent E. Burnout-depression overlap: a
review. Clin Psychol Rev 2015; 36: 28–41.
6. Leiter M, Durup J. The discriminant validity of burnout and
depression: a confirmatory factor analytic study. Anxiety Stress
Coping 1994; 7: 357–73.
7. Wurm W, Vogel K, Holl A et al. Depression-burnout overlap in
physicians. PLoS ONE 2016; 11.
8. Bridgeman PJ, Bridgeman MB, Barone J. Burnout syndrome among
healthcare professionals. Am J Health Syst Pharm.
2018;75(3):147-152.
9. D Coghlan. Phases of burnout among Irish professionals. J Health
Hum Serv Adm 1999;22(1):16-23.
10. CP West, LN Dyrbye, TD Shanafelt . Physician burnout:
contributors, consequences and solutions. J Intern Med; 2018;
283(6): 516- 529.
11. Isabelle Roy Burnout syndrome: definition, typology and
management.iscrpljenost Soins Psychiatr.2018; 39 (318): 12-19.
12. De Simone S, Vargas M, Servillo G. Organizational strategies to
reduce physician burnou: a systematic review and meta-analysis.
Aging Clin Exp Res. 2021;33(4): 883-894.
13. Malinauskas R, Grinevicius G, Malinauskiene V. Burnout among
Telecommunication Sales Managers. Int J Environ Res Public Health;19
(18) :11249.
14. Tehrani Sh, , Keshtkar A, Ramasamy A, Fadaei M. The worldwide
prevalence of burnout syndrome among bank employees: a systematic
review and meta-analysis protocol Syst Rev; 2021 ;10 (1): 283.
15. Wuttipat Kiratipaisarl, Vithawat Surawattanasakul, Wachiranun
Sirikul. Individual and organizational interventions to reduce
burnout in resident physicians: a systematic review and
meta-analysis. BMC Med Educ 2024; 24:1234.
16. Tamara D Street, Sarah J Lacey, Klaire Somoray. Employee Stress,
Reduced Productivity, and Interest in a Workplace Health Program: A
Case Study from the Australian Mining Industry Int J Environ Res
Public Health. 2018 Dec 31;16(1): 94.
17. Gómez-Urquiza HL, De la Fuente-Solana E, Albendín-García L,
Vargas-Pecino C, Ortega-Campos E, Cañadas-De la Fuente G .
Prevalence of Burnout Syndrome in Emergency Nurses: A Meta-Analysis.
2017; 37(5): 1-9.
18. Ying Y, Hayes J. Causes and consequences of burnout among mental
health professionals: A practice-oriented review of recent empirical
literature Psychotherapy 2020;57(3):426-436.
19. Parker G, Tavella G. The Diagnosis of Burnout: Some Challenges J
Nerv Ment Dis; 2021;210 (7): 475-478.
20. Woo T, Ho R, Tang A, Tam W. Global prevalence of burnout
symptoms among nurses: A systematic review and meta-analysis; J
Psychiatr Res; 2020; 123: 9-20.
21. Williams ES, Manwell LB, Konrad TR, Linzer M. The relationship
of organizational culture, stress, satisfaction, and burnout with
physician-reported error and suboptimal patient care: results from
the MEMO study. Health Care Manage Rev 2007; 32: 203–12.
22. Ovchinniko YV, Palchenkova MV, Kalachev OV. Burnout syndrome:
diagnosis, principles of treatment, prophylaxis. Voen Med Zh; 2015;
336 (7): 17-24.
|
|
|
|