|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
Page 119 |
||||||||||||||||||||||||||||||||||||
|
Case report Disconnection of arterial collateral as the cause of lower leg amputation after conquassation caused by petrol tiller. A case report Ivan Golubović (1), Predrag Stojiljković (1), Mihailo Ille (2), Milan Radojković (3), Nemanja Jovanović (3), Milan Lazarević, Ivana Golubović (3), Ivan Milošević (2), Zoran Baščarević (4), Dejan Tabaković (5), Nebojša Mitić (1)CLINIC FOR ORTHOPAEDIC SURGERY AND TRAUMATOLOGY, CLINICAL CENTER NIS, SERBIA; (2)CLINIC FOR ORTHOPAEDIC SURGERY AND TRAUMATOLOGY, CLINICAL CENTER BELGRADE, SERBIA; (3)FACULTY OF MEDICINE, UNIVERSITY OF NIS, SERBIA; (4)INSTITUTE OF ORTHOPAEDIC SURGERY “BANJICA”, BELGRADE, SERBIA; (5)CLINIC FOR ORTHOPAEDIC SURGERY AND TRAUMATOLOGY, CLINICAL CENTER KOSOVSKA MITROVICA, SERBIA |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Download in pdf format | ABSTRACT:
Introduction. Leg conquassationconquassation caused by petrol tiller
is one of the most severe injuries in bone and joint traumatology.
Firm strokes by sharp tiller blades produce strong force that easily
damages both soft tissues and bones. Since tillers are used in soil
processing, the wounds are highly contaminated with dirt and
fertilizers, hence the anaerobic spore-forming bacilli, such as
tetanus and gas gangrene pathogens. Casereport. This paper presents
the treatment of a 69 years old man with chronic arterial
insufficiency of the lower extremities who suffered severe injury of
the lower leg (IIIB open tibial fracture according to Gustillo) by
petrol tiller while performing agricultural work. Due to the absence
of pulsations, Multislice CT angiography and arteriography were
performed. Arteriography of the injured leg confirmed chronic
occlusion of the anterior tibial artery and numerous stenotic
lesions of the peroneal and posterior tibial arteries. Posterior
tibial artery was chronically occluded in its distal part and
connected to the foot with moderately developed collateral arteries
which provided the viability of the injured leg. Despite undertaken
basic principles of treatment of this serious injury (primary
surgical treatment of wounds, external fixation, reconstruction of
soft tissue, antibiotic and anti-tetanus prophylaxis) due to
infection and gangrene the treatment ended with lower leg
amputation. Conclusion. Leg amputation can be expected in this type
of injuries in cases of extensive destruction of tissue in the field
of existing chronic arterial insufficiency in elderly patients, even
in the absence of injury of main blood vessels due to traumatic
disconnection of collateral in such patients. Keywords: leg conquassation, IIIB open tibial fracture, external fixation, chronic arterial insufficiency, amputation of the lower leg |
|||||||||||||||||||||||||||||||||||
INTRODUCTIONFarmer is one of the most frequent professions in Serbia. Leg
conquassation caused by engine tiller is among the most severe
injuries in bone and joint traumatology. Firm strokes produced by
sharp tiller blades produce strong force that easily damages both
soft tissues and bones. Since tillers are used in soil processing,
the wounds are highly contaminated with dirt and fertilizers, hence
the anaerobic spore-forming bacilli, such as tetanus and gas
gangrene pathogens. Skin and soft tissue destruction, comminution
and bone defect, high level of both anaerobic and aerobic
contamination and threatening infection make the treatment of these
injuries, particularly open lower leg fracture, complex and
challenging (1). CASE REPORTA 69-year old male patient was injured during soil processing by
an engine tiller when the machine hit the hurdle in the ground,
changed the direction and caused him severe both right and left
lower legs and feet trauma with its sharp blades. Injuries included
open left lower leg fracture Gustilo type IIIB with soft tissue
defect, severe laceration of the left foot dorsum also with soft
tissue defect and right lower leg laceration. He was initially
admitted to the regional hospital emergency unit where his injuries
were assessed and left leg plaster immobilization was done.
Subsequently, the patient was referred to Orthopaedics and
Traumatology Clinic, Clinical Center Nis where resuscitation and
preoperative preparation were immediately performed. On examination,
there was large skin and subcutaneous tissue defect on the front
left lower leg with lacerated and ruptured tibialis anterior muscle
tendon. X-rays revealed comminuted fracture of the left lower leg
proximal third and left medial malleolus fracture. Left lower leg
was deformed in the proximal third with complete functional
impairment. There were crepitations during the movements and
palpation of the fracture site. Both anterior and posterior tibial
pulses were absent. Figure1. Multislice CT angiography of injured lower leg
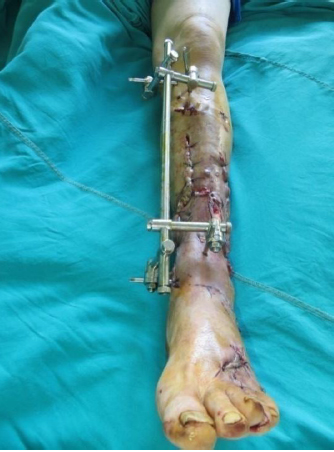
Figure 2. Left lower leg after the primary wound care and external skeletal fixation.
The patient was administered anti-tetanus protection and
anticoagulant prophylaxis of deep vein thrombosis and pulmonary
thromboembolism (nadroparin 0,6mL/24hr). The patient received
postoperative intravenous antibiotic therapy (ceftriaxone 2gr daily,
amikacin 500mg/12hr and metronidazole 500mg/8hr). Vascular surgeon
administered the medication therapy for chronic arterial
insufficiency of the lower extremities. Figure 4. Front left lower leg and foot dorsum soft tissue necrosis with the dry gangrene of the third finger.
Secondary wound debridement including necrosectomy and gangrenous third finger of the left foot amputation was performed in spinal anesthesia (Figure 5). Figure 5. Left lower leg and foot after secondary wound debridement including necrosectomy and gangrenous third finger amputation
It was followed by general aggravation, severe wound infection, infection around the skeletal fixator nails and critical lower leg ischemia. A multidisciplinary team of orthopedist, vascular and plastic surgeons made a decision to amputate the lower leg for vital indication (Figure 6). Figure 6. Severe infection of the amputation stump.
Perioperatively, the patient was administered 1750mL whole blood transfusion and 1500mL fresh frozen plasma. Postoperatively it was continued with antibiotics (ceftriaxone 2gr daily, clindamycin 600mg/12hr and vancomycin 1gr/12hr) and subcutaneous anticoagulant (nadroparin 0,6mL/24hr). Meticulous everyday wound cleaning and dressing was performed. However, infection and necrosis of the amputation stump developed. All the sutures were removed, debridement of the stump was done and it was left wide open. Thorough everyday wound care was continued. Seven days after the amputation secondary debridement of the stump and wound closure were performed (Figure 7). Postoperative course was uneventful. The stump healed and the sutures were removed. The patient was referred to physical therapy and limb prosthesis specialist. Figure 7. Amputation stump after repeated debridement and secondary wound closure
DISCUSSIONAgriculture is one of the most important economy braches in
Serbia. Limb injuries caused by petrol tiller almost always include
sever skin and soft tissue destruction, magistral blood vessels
injury, severe comminuted fracture and often traumatic amputation.
These injuries are highly mutilating and may lead to death.
Possibilities of tissue reconstruction are small and require
multidisciplinary approach that includes orthopedist, vascular and
plastic surgeons. CONCLUSIONLeg amputation, can be expected in conquassant lower leg injuries
in cases of extensive destruction of tissue in the field of existing
chronic arterial insufficiency in elderly patients, even in the
absence of injury of main blood vessels due to traumatic
disconnection of collateral. LITERATURE:
|
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| [
Contents
] [ INDEX ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||