|
||||||||||||||||||||||||||||||||||||
| [ Sadržaj
] [ Indeks autora ]
|
||||||||||||||||||||||||||||||||||||
| UDK 613-056.24:616.341-008.1-053.2 COBISS.SR-ID 276240652 |
ISSN 0350-2899. - Vol. 44, br. 1 (2019), |
|||||||||||||||||||||||||||||||||||
|
Originalni rad / Original paper Self-assessment and parental
assessment of quality of life children with coeliac disease Biljana Stojanović –Jovanović (1),
Stevan Jovanović (1), Biljana Vuletić (2) |
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Preuzmite rad u pdf formatu | Summary: Background:
Celiac disease is a chronic autoimmune disease characterized by
intolerance to gluten. Treatment is carried out by strict lifelong
gluten-free diet. Study aims to determine the quality of life
children and adolescents with celiac disease who are on controlled
diet, based on self-assessment and proxy assessment by their
parents. Methods: The study included 116 children and adolescents
diagnosed with celiac disease who are on a gluten free diet for at
least one year and the same number of their parents. The children
were aged 5 to 18 years. The patients and their parents were
recruited at the Institute for Maternal and Childs healthcare of
Serbia and the University Children's Hospital in Belgrade. The used
instruments were a child and parent version of the Pediatric Quality
of Life Inventory and the Screen for Child Anxiety Related Disorder.
Results: The results in both versions of the questionnaires
Pediatric Quality of Life Inventory showed similar values. (P> 0.05,
all analyzes). There was a greater value of three scores in
instrument named Screen for Child Anxiety Related Disorder
(questionnaire for children) compared to (questionnaire for
parents). These are the total score (p<0.05), separation anxiety
(p<0.01) and the avoidance of the school (p<0.05). Conclusions:
Disagreement between the children's selfassessment and parental
assessment, justifies the importance of hearing subjective
children's opinion on their quality of life as well as of their
parents. This research has given us information about some of the
critical points by which we can focus future studies. Key words: Celiac disease, children, gluten, diet, quality of life. Sažetak: Celijakija je hronična autoimuna bolest
koju karakteriše netolerancija na gluten. Lečenje se vrši striktnom
doživotnom dijetom bez glutena. Cilj rada je da se utvrdi kvalitet
života dece i adolescenata sa celijakijom koji su na kontrolisanoj
ishrani, na osnovu samoprocene i procene od strane roditelja.
Metode: Istraživanje je obuhvatilo 116 dece i adolescenata sa
dijagnozom celijakije koji su na dijeti bez glutena najmanje godinu
dana i isto toliko roditelja. Deca su uzrasta od 5 do 18 godina.
Istaraživanje je realizovano u Institutu za zdravstvenu zaštitu
majke i deteta Srbije i Univerzitetskoj dečjoj klinici u Beogradu.
Korišćeni instrumenti su dečija i roditeljska verzija Pedijatrijskog
upitnika za procenu kvaliteta života (PedsQL) i Upitnika za pretragu
anksioznih poremećaja kod dece (SCARED). Rezultati: Rezultati u obe
verzije Pedijatrijskog upitnika za procenu kvaliteta života pokazali
su slične vrednosti (P> 0,05, sve analize). Rezultati procene
prisustva anksioznih poremećaja na dečjoj verziji SCARED skale,
pokazuju statistički značajno veću vrednost tri skora u odnosu na
procenu njihovih roditelja. To su, Ukupan skor (p < 0,05), Socijalna
anksioznost (p < 0,01) i Izbegavanje škole (p < 0,05). Zaključak:
Život sa celijakijom i bezglutenskom ishranom može biti težak za
decu i adolescente jer se osećaju da su drugačiji od svojih vršnjaka
zbog čega redukuju druženja i izoluju se. U ovoj studiji došli smo
do saznanja da deca i adolescenti sa celijakijom imaju značajno niži
ukupni QOL i to kako na osnovu samoprocene tako i na osnovu
roditeljske procene. |
|||||||||||||||||||||||||||||||||||
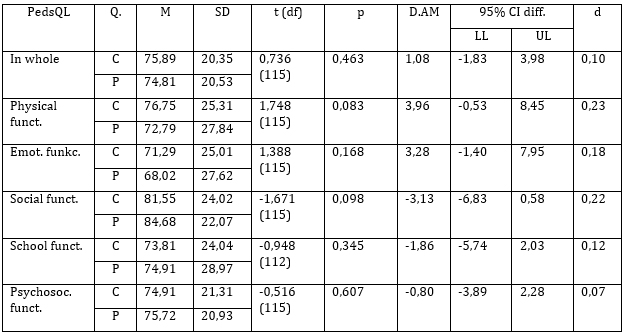
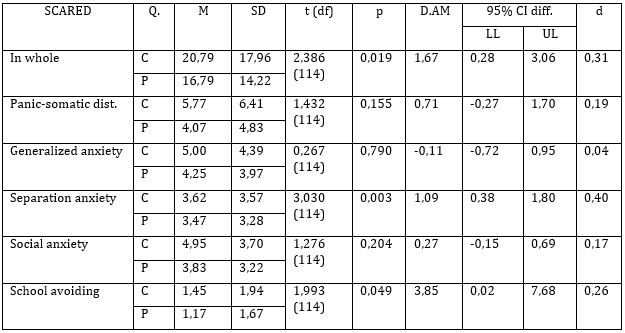
INTRODUCTIONEvaluation of the quality of life of the patients in general and therefore patients with celiac disease has become the practice of the past half century [1]. Celiac disease is an autoimmune disorder caused by the ingestion of gluten in persons who have a hereditary predisposition for this disease. It is a chronic, multi-organ disease in which is present a different degree of damage of the small bowel mucosa and the different spectrum of clinical symptoms [2]. Chronically ill children are more prone to physical, psychological, social problems than healthy children and that can affect the child's quality of life in relation to health in a negative way [3]. Early diagnosis of celiac disease reduces complications and contributes to a positive attitude towards the disease. Strict lifelong gluten-free diet with no peptides of wheat, barley, oats and rye is the only known treatment method [4]. Gluten-free diet can cause problems in the acceptance by the child and his family [5]. Children who are on a gluten free diet for a long time, often break the diet during their adolescence. An important factor of disrespect of restrictive diet in adolescence is a peer pressure, unclear labeling of food and bustling lifestyle of teenagers [6]. Research shows, that it is important for parents to accept the illness of their children because it has a positive impact on a child to accept its own disease easier [7]. Some studies confirm the high incidence of psychological problems such as anxiety, as problems of adaptation to the social life of children who are on a strict diet without gluten [8]. The problems are particularly pronounced in children of school age. This, because it is a period in which is important for the child not to be different from the other children[9]. Measuring quality of life in children, includes physical and psychosocial aspects, as well as individual health assessment [10]. There are studies that show differences in experience of the health quality of life between parents and their children [11]. Therefore, previous studies indicate that for the assessment of children 's quality of life is the most appropriate to use a double approach, and children's opinion to supplement by the opinion of parents [12]. Therefore, in this study we aim to determine the quality of life of Serbian children and adolescents with celiac disease who are on controlled diet, based on self-assessment and proxy assessment by their parents. METHODSParticipants Description of used instruments Ethical considerations Statistical Analysis RESULTSThe study included a total of 116 children and adolescents aged 5 to 18 who have a diagnosis of celiac disease and 116 parents (one parent of each child). Demographic and clinical features of patients are given in Table 1. Tabela 1. Opšte demografske karakteristike grupa Tabela 2. Struktura uzorka ispitivanih roditelja Note: Number of respondents (n = 116); Note: Q. - Questionnaire; C - for a child; P - for parent Note: Q. - Questionnaire; C - for a child; P - for parents; DISCUSSIONEach chronic disease and thus celiac disease, which if occurs in children during the period of their growth and development can affect the psychosocial development, self-perception, self-esteem, social functioning, and finally in a few studies have been found to significantly affect health related quality of life of children and adolescents [15]. In our study, children and adolscents with celiac disease and their parents gave similar answers in the pediatric questionnaire about quality of life (PedsQL), so all observed scores statistically were homogeneous. Our results are consistent with the results of European studies in which the evaluation of self-assessment of the quality of life of children and adolescents with celiac disease and assessment of their parents shows that the disease does not have significant negative impact on quality of life [16]. Unlike our results, other studies have found that parents have significantly poorer perception of health related quality of life of their children than the children themselves [15,17]. In our study, comparing the assessment of children and adolescents with celiac disease with the assessment of their parents on screening emotional problems, we get a significantly higher value of three scores SCARED (questionnaire for the child in relation to the SCARED (questionnaire for parents). These are the total score (p <0.05), separation anxiety (p <0.01) and the school avoidance (p <0.05). The results of several studies suggest that children and adolescents with celiac disease recorded high incidence of psychological problems such as anxiety, depression, fears, feelings of sadness and low tolerance for frustration, emotional hypersensitivity, shyness, irritability and showing problems of adaptation to social life. Children and adolescents avoid socializing with peers, they abstain to take meals with others outside the home and therefore can alienate [18,19]. Since the school environment and peers are having very important role in the normal development and functioning of children, adaptation to school work and peer groups is a significant indicator of the functioning of children and adolescents who have a chronic disease and are on specific dietary treatment. Due to the specific disease and strict diets, children and adolescents absent from school, missing several weeks of classes and lose contact with their peers and peer activities and interactions. Results of some studies that have had to examine the impact of chronic disease on the behavior of children, show that the examined children present concern about the absence from school, separation from peers, the feeling of diversity, increased need for care and helping loved ones [20]. Schools and teachers should work with parents and to support children with these and other problems. It is necessary that teachers and peers improve their knowledge about celiac disease because children spend a large part of their time in schools under their control and interaction. The results of our study are consistent with previous studies that have dealt with this theme, showing that children and adolescents who suffer from celiac disease lack psychological support to overcome the problems they face [21, 22]. CONCLUSIONIncomplete agreement between self and proxy-assessment justifies
the importance of considering the opinion on quality of life from
both, children and their parents. Respect of gluten-free dietary
regime is an essential factor for obtaining optimal quality of life
in relation to health. Children with celiac disease need the support
of their families in respecting of gluten-free diet. It is necessary
to provide psychosocial and educational support for children and
adolescents who have difficulty to strictly adhere to the regime
gluten-free diet and this is a task not only for parents but for
teachers and health workers. ZAKLJUČAKNepotpuna usaglašenost između samoprocene i roditeljske procene kvaliteta života dece sa celijakijom, opravdava značaj i potrebu, uzimanja u obzir mišljenja o ovome i od same dece i njihovih roditelja. Poštovanje dijetalnog, bezglutenskog režima ishrane je osnovni faktor za postizanje optimalnog kvaliteta života u vezi sa zdravljem. Deci i adolescentima sa celijačnom bolešću neophodno je obezbediti psihosocijalnu i obrazovnu podršku u striktnom pridržavanju bezglutenskog režima ishrane a to je zadatak ne samo za roditelje već i za nastavnike i zdravstvene radnike. REFERENCES
|
||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||
| Adresa autora / Corresponding
address: Biljana Stojanović - Jovanović, Higher Education School of Professional Health Studies, Belgrade E-mail: biljananstojanovic@gmail.com |
Rad primljen: 20.2.2019. Elektronska verzija objavljena: 13.5.2019. |
|||||||||||||||||||||||||||||||||||
| [ Sadržaj
] [ Indeks autora ]
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||