| |
|
|
INTRODUCTION
In Serbia, only three species of venomous snakes exist, each with
one or two subspecies: the nose-horned viper (Vipera ammodytes), the
adder (V. berus), and the meadow viper (V. ursinii) [1-4]. All are
strictly protected or protected by law [5]. In our country,
including the surroundings of the city of Vršac (Banat region,
Vojvodina province, northeastern Serbia), the Balkan adder, Vipera
berus subsp. bosniensis occurs (Figure 1A,B) [1,2,6]. Another viper,
V. ammodytes, widely distributed south of the Danube and Sava
rivers, also was recorded approximately 40 kilometers to the south
from Vršac [7]. The experts did not exclude the possibility that in
rare remnants of steppe habitats in Vojvodina the third viper
occurs, V. ursinii, subsp. rakosiensis [1].
Figure 1. Vipera berus bosniensis from the Vršačke
planine Mts.: A) an adult in the open, and B) a specimen well hidden
in dry grass (Photos: Milivoj Krstić).
Slika 1. Vipera berus bosniensis sa Vršačkih planina: A) odrasla
jedinka na otvorenom i B) jedinka dobro sakrivena u suvoj travi
(Fotografije: Milivoj Krstić).

According to the World Health Organization, two of the vipers
present in Serbia are medicinally important – the nose-horned viper
and the adder; the meadow viper is only moderately harmful to humans
[8].
The venoms of adder and nose-horned viper differ in composition and
effects [9]. Neurotoxic effects of adder venom are known for a long
time, as are the differences in venom composition and in
consequences of envenomation between two of the adder subspecies
present in the Balkans, V. b. berus and V. b. bosniensis [10,11].
Resulting from the distribution patterns of the species, bites by V.
ammodytes are more frequent than those by V. berus in all
ex-Yugoslav countries for which the overview publications could be
found [Nikolić, unpublished].
In Serbia, bites by venomous snakes do occur every year [Nikolić,
unpublished], but their analyses are not being performed and made
publicly available. A central register of the incidences of venomous
snakebites still does not exist in Serbia: its making was initiated
only in 2018, and the collected data were not available at the time
of this manuscript preparation [12].
In general, published information concerning the bites of Vipera b.
bosniensis are almost inexistent. Detailed case reports from the
neighboring countries date back only to the 2010s [11,13,14]. On the
other hand, the first adder bites in Vojvodina were described by a
medical professional already in 1901 [15], although from the Fruška
gora Mt., Srem region. Only one publication was found regarding
adder bites in the Vršac area, presenting six cases [16]. Between
these two reports, a 100-years gap exists. After the year 2000,
nothing of a kind was published for Vojvodina: several other cases
previously treated in the Vršac hospital were not presented in the
scientific literature. In general, in Serbia, only two additional
publications were found concerning venomous snakebites, regarding V.
ammodytes [17,18]. Importantly, no fatal outcomes were recorded.
People often cannot recognize snake species, but in our case, no
doubts existed regarding the identification of the “culprit”: the
professional was bitten, who clearly recognized the species.
With this case report, we intended to contribute to the collecting
and publishing of the data regarding the seriously neglected
venomous snakebites.
CASE REPORT
On April 25, 2019 at around 10:40 a.m., one of the authors, an
experienced 43-year old field investigator, ranger in the Landscape
of Outstanding Features “Vršačke planine”, encountered an adder and
wanted to photograph it, for the documentation. It was a sub-adult
almost melanistic male (Figure 2A). Although well aware of the
potential threat and despite handling the snake with due caution,
for a moment his attention dropped and the snake bit him at the tip
of his left-hand middle finger. The single fang only scratched the
skin under the nail (Figure 2B).
Figure 2. A) The snake that inflicted the bite; B)
tip of the patient’s left-hand middle finger a week after the bite
(Photos: Milivoj Vučanović).
Slika 2. A) Zmija koja je nanela ujed; B) vrh srednjeg prsta leve
ruke pacijenta nedelju dana nakon ujeda (Fotografije: Milivoj
Vučanović).

The patient squeezed and intuitively sucked the bite wound and
probably ingested a bit of venom. During the first ten minutes,
there was no reaction to the bite. After those ten minutes, “an
initially unidentifiable change in the body” was felt. The injured
man started driving his car towards the hospital by himself but
accompanied by a colleague. Along the way he felt sudden exhaustion
and noted that the colors of the surroundings had changed, i.e.
brightened (the sky was brightly shining, leaves turned fluorescent
green, the road shimmered like ice). The hospital was reached after
about 35 minutes.
On admission, approximately 40 minutes after the bite, the patient
was sweating and he complained of nausea and exhaustion but was able
to explain what happened. He sat on the chair and vomited for the
first time. Since he was unable to stand alone, he was put in a
wheelchair. While being driven to the Infectious diseases
department, he was unable to keep his feet lifted.
Of average osteomuscular build, he was conscious, oriented in space,
time and towards faces, afebrile, acyanotic, anicteric, eupneic at
rest, with no signs of hemorrhagic syndrome. His systolic blood
pressure was 80 mmHg, but the diastolic was immeasurable. He denied
chronic diseases and allergies to medications; he is a non-smoker
and does not consume alcohol. During the admission, the patient
vomited watery contents twice but he did not have diarrhea. Physical
findings on head and neck were normal; there was no strabismus or
diplopia. Auscultation showed normal breath sounds, cardiac action
was rhythmic with clear tones; TA 80/NA (still immeasurable) mmHg.
The abdomen was soft, insensitive on palpation; liver at right
costal margin, renal succussion negative. There was no swelling or
deformities on extremities, only the bitten finger was slightly
hyperemic: although the bite mark was not visible, minor swelling
and redness developed at the place of bite. The patient had no
neurologic deficits; meningeal signs were negative. Slight ptosis of
the left eyelid developed. After being put to bed, the patient
vomited three more times and had mild but uncontrollable diarrhea.
He was conscious but was too weak to talk or keep his eyes open.
Immediately after the admission, the patient received the
antihistamine Synopen (hloropiramin) i.v., and Lemod-Solu
(metilprednizolon) 80 mg. Intravenous infusions were introduced –
sol NaCl (natrii chloridi infundibile) 0.9% 500.0, sol Dextrosae
(glucose) 5% 500.0, and the Jugocilin (benzilpenicilin-prokain)
antibiotic 1,600,000IU was given i.m.
A single dose (5 ml) of the equine viper venom antiserum Viekvin®
was administered i.m. at 11:45 a.m., approximately 65 min after the
bite, at the place of bite on the hand and in the forearm. After an
hour, the patient started feeling better.
At 12:20 p.m. tension still 80/NA mmHg; infusion application
continued (sol NaCl 0.9% and sol Dextrosae 5%). Slight ptosis of the
left eyelid became evident. The patient appeared drowsy, his talk
was slow and slurry. Nevertheless, after two hours, all sensations
were back to normal, and the patient felt good, except he could not
control his eyelids.
At 13:20 p.m., the patient felt better, with TA 120/70 mmHg and
diuresis of 350 ml (the single instance from the admission, at 13
p.m.). During the afternoon the ptosis of both eyelids developed: he
could not open the eyes.
At 18:30 p.m. the patient’s TA was 140/100 mmHg. At 22:00 p.m. TA
was unchanged, and body temperature was 37.5°C. The patient was
stable.
During the first day in the hospital, the patient was given 3 l of
liquid i.v. He was not given anti-tetanus protection because he had
already received the third dose of Tetalpan in February 2018, i.e.
he was regularly vaccinated previously.
On April 26, the patient felt well, his TA was 120/80 mmHg and
diuresis 2.250 ml (from admission until 6 a.m.). Ptosis was less
prominent than on the previous day. Physical findings were normal.
On the third day, April 27, ptosis was still present but weaker: the
patient could keep his eyes open, but still did not completely
regain eyesight. Findings on the place of the bite were normal.
On April 28, ptosis receded almost completely; the patient had no
objective sight problems. On April 29, the ptosis receded
completely.
The patient was released from the hospital on April 30, the sixth
day after the bite. Although clinically well, his sight did not
fully recover: he still had trouble “sharpening” images for a couple
of seconds after turning his head. In addition, after two or three
hours of activity, his head would start aching. Subjectively, he
fully recovered after 10–12 days. The bitten fingertip remained numb
for about a month.
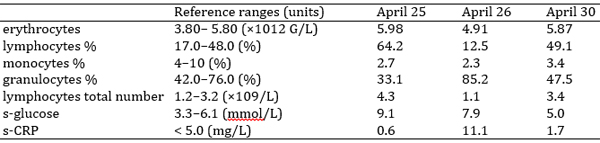
Laboratory tests: Laboratory analyses were performed at the
admission, on the second day of hospitalization and before the
patient was released. Values of the tests that departed from normal
are provided in Table 1. Other hematological, biochemical and
hemostatic parameters were within their reference ranges. Urine was
tested only on the second day, and all parameters were
normal/negative (pH, density, appearance, color, blood, bilirubin
and urobilinogen, leucocytes, ketones, proteins, nitrites, and
glucose).
Table 1. Results of laboratory analyses during the
course of hospitalization. Elevated values are given in boldface,
lowered are italicized.
Tabela 1. Rezultati laboratorijskih analiza vršenih tokom
hospitalizacije. Povišene vrednosti su podebljane, a snižene
iskošene.
DISCUSSION
Although previously healthy and practically merely scratched on
the finger with only one snake’s fang, the patient experienced
moderately severe envenomation and spent six days in the hospital.
He encountered a snake in a place that is not isolated: weekend
house owners regularly use the road he took that day – mostly in
cars, but also on foot; other types of visitors are also quite
usual. Vipera b. bosniensis is long known for its potent neurotoxic
venom, and reactions to its bites similar to the one we described
were reported from Croatia, Bulgaria, and Hungary, in addition to
the previous six cases from the Vršac hospital [11,13,14,16].
Although sometimes causing severe clinical pictures, adder bites are
rarely fatal [e.g. 19]. Importantly, the antivenin manufactured in
Serbia is effective in the cases of adder bites, although it is made
from the venom of Vipera ammodytes [17,20].
Our laboratory analyses of blood and urine did not show dramatic
aberrations from reference values. Varga et al. [14] provided a list
of papers presenting and discussing laboratory findings in the cases
of V. berus bites: among the previously reported, we found elevated
levels of glucose and CRP. We also had increases in erythrocytes,
but lowered monocytes %, while the numbers/percentages of lympho-
and granulocytes oscillated from below to above the reference
ranges. Systemic symptoms did develop but did not last for long. The
only persistent effects were problems with eyes – blepharoptosis and
vision impairment.
The cases of adder bites previously described from the surroundings
of Vršac [16] were similar to the one we reported of here. Of the
six patients treated during 18 years, three got bitten to the
fingers while attempting to catch the snakes; two sucked the wound
and one squeezed it (the remaining three did not apply the first
aid). Both local and systemic symptoms were mild to moderate, with
complications in a person suffering from asthma. All patients (22–57
years of age) received antivenin within 30 min to 4 hours after the
bite, and they spent 2–8 (4.8 on average) days in the hospital.
In general, adder bites in the surroundings of Vršac are not
frequent and they are surely not lethal, as the media like to
present them, using the phrases like “he barely survived the attack
of a snake”.
Vršačke planine Mts. are one of only several remaining lowland/hilly
habitats of Vipera berus in Serbia [1,6,21]. Like in its other
non-mountainous habitats, due to the constant spreading of human
influences, the adder is often found near the settlements and arable
land [21]. This makes it vulnerable to various anthropogenic
influences [6] and poses the potential threat to people. In Serbia,
the species is strictly protected by national legislation and was
recently designated as vulnerable; the prescribed fine for its
killing is 100.000 dinars (app. 850 €) [2,5,22].
In our case, the snake bit an experienced and cautious person, a
professional biologist, who was aware that his own mistake during
the handling of the animal led to the bite. Laypeople either fear
snakes enough to wish to kill them all, or they want to show off
trying to catch or/and torture them. Those are the situations in
which many of the bites occur [16,23,24].
CONCLUSION
Although the distribution of vipers in Serbia is comparatively
well explored, some new populations of all three species might be
“discovered” in suitable habitats, like in e.g. Hungary [25]. The
exchange of information is necessary among scientists (professionals
in biology and medicine), and between the experts and the general
public, including the media. With humble effort, proper education
could be provided to the target population and the risk of
snakebites could be minimized.
Acknowledgements
Sonja Nikolić is financed through the Project No. 173043 of the
Ministry of Education, Sciences and Technological Development of the
Republic of Serbia. Milivoj Krstić kindly allowed us to use his
photographs of the adders from the Vršačke planine Mts. This study
did not receive any specific funding. We are grateful to the
anonymous reviewer whose constructive critique and comments helped
us improve the manuscript.
Conflicts of interest
None.
REFERENCES
- Jelić D, Ajtić R, Sterijovski B, Crnobrnja-Isailović J, Lelo
S,Tomović L. Distribution of the genus Vipera in the western and
central Balkans (Squamata: Serpentes: Viperidae). Herpetozoa
2013; 25 (3/4): 109–32.
- Ajtić R, Tomović L. Vipera berus (Linnaeus, 1758). In:
Tomović L, Kalezić M, Džukić G, editors. Red book of fauna of
Serbia II – Reptiles. University of Belgrade, Faculty of
Biology, and Institute for Nature Conservation of Serbia,
Belgrade; 2015. p. 241–7.
- Tomović L. Vipera ammodytes (Linnaeus, 1758). In: Tomović L,
Kalezić M, Džukić G, editors. Red book of fauna of Serbia II –
Reptiles. University of Belgrade, Faculty of Biology, and
Institute for Nature Conservation of Serbia, Belgrade; 2015. p.
233–9.
- Tomović L, Ajtić R. Vipera ursinii (Bonaparte, 1835). In:
Tomović L, Kalezić M, Džukić G, editors. Red book of fauna of
Serbia II – Reptiles. University of Belgrade, Faculty of
Biology, and Institute for Nature Conservation of Serbia,
Belgrade; 2015. p. 249–54.
- Anonymous. Pravilnik o proglašenju i zaštiti strogo
zaštićenih i zaštićenih divljih vrsta biljaka, životinja i
gljiva [Regulation on the designation and conservation of the
strictly protected and protected wild species of plants, animals
and fungi]. Službeni glasnik Republike Srbije [Official Gazette
of the Republic of Serbia] 2011; Nos. 5/2010 and 47/2011.
- Tomović L, Ajtić R, Ljubisavljević K, Urošević A, Jović D,
Krizmanić I, et al. Reptiles in Serbia – Distribution and
diversity patterns. Bull Nat Hist Mus Belgr 2014; 7: 129–58.
https://doi.org/10.5937/bnhmb1407129T
- 7. Džukić G, Kalezić M, Marković M. Poskok (Vipera
ammodytes) – autohtona zmija Vojvodine! [Nose-horned viper
(Vipera ammodytes) – autochthonous snake in Vojvodina!] Godišnji
bilten Prirodnjačkog društva Gea 2005; 5: 13.
- WHO – World Health Organization. Health Systems and
Services: Quality and Safety of Medicines – Blood Products and
related Biologicals. Available at
http://apps.who.int/bloodproducts/snakeantivenoms/database/default.htm
(Last accessed on 11 September 2019).
- Latinović Z, Leonardi A, Šribar J, Sajevic T, Žužek MC,
Frangež R. et al. Venomics of Vipera berus berus to explain
differences in pathology elicited by Vipera ammodytes ammodytes
envenomation: Therapeutic implications. J Proteomics 2016; 146:
34–47.
https://doi.org/10.1016/j.jprot.2016.06.020
- Radovanović M, Martino K. Zmije Balkanskog poluostrva.
Srpska akademija nauka, Naučno-popularni spisi, Knjiga 1;
Institut za ekologiju i biogeografiju, Knjiga 1. [Snakes of the
Balkan Peninsula. Serbian Academy of Sciences,
Scientific-popular writings, Book 1. Institute for Ecology and
Biogeography, Book 1] Naučna knjiga, Belgrade. 1950: p. 43.
- Malina T, Krecsák L, Jelić D, Maretić T, Tóth T, Šiško M. et
al. First clinical experiences about the neurotoxic envenomings
inflicted by lowland populations of the Balkan adder, Vipera
berus bosniensis. NeuroToxicology 2011; 32: 68–74.
https://doi.org/10.1016/j.neuro.2010.11.007
- Dobaja Borak M, Babić Ž, Bekjarovski N, Cagánova B, Grenc D,
Gruzdyte L. et al. Epidemiology of Viperidae snake envenoming in
central and south-eastern Europe: CEE Viper Study. In: Abstracts
from the 39th International Congress of the European Association
of Poisons Centres and Clinical Toxicologists (EAPCCT) 21–24 May
2019, Naples, Italy. Clin Toxicol 2019; 57(6): 470.
- Westerström A, Petrov B, Tzankov N. Envenoming following
bites by the Balkan adder Vipera berus bosniensis – First
documented case series from Bulgaria. Toxicon 2010; 56: 1510–5.
https://doi.org/10.1016/j.toxicon.2010.08.012
- 14. Varga C, Malina T, Alföldi V, Bilics G, Nagy F, Oláh T.
Extending knowledge of the clinical picture of Balkan adder
(Vipera berus bosniensis) envenoming: The first
photographically-documented neurotoxic case from South-Western
Hungary. Toxicon 2018; 143: 29–35.
https://doi:10.1016/j.toxicon.2017.12.053
- Mirković S. Kako prost narod u Fruškoj gori i Sriemu lieči
rane nastale ujedom otrovnih zmija [How laypeople in Fruška gora
and Sriem heal the wounds resulting from venomous snake bites]
Liečnički Viestnik 1901; 23: 246–8. [In Serbian].
- Častven J, Šinžar T, Kovačević D, Moroanka E, Mitrović D,
Stanivuković M. Zmijski ujedi u području Vršačkih planina –
prikaz slučajeva [Snakebites in the region of Vršac mountains –
case reports]. Acta Infectologica Yugoslavica 2000; 5: 75–82.
[In Serbian with summary in English]
- Milićević M. Prikaz bolesnika ujedenih od otrovnih zmija
lečenih od 1960. do 1968. godine / Vorstellung der Kranken die
von Giftschlangenbissen im Jahre 1960 bis 1968 behandelt wurden
[Presentation of the patients bitten by venomous snakes treated
between 1960 and 1968]. Srpski arhiv za celokupno lekarstvo1968;
96(10): 999–1006. [In Serbian with summary in German].
- Stojanović M, Stojanović D, Živković Lj, Živković D.
Hemoragijski sindrom kod zmijskog ujeda [Hemorrhagic syndrome in
snakebite]. Apollineum Medicum et Aesculapium 2007; 5(3-4):
8–10. [In Serbian with summary in English]
- Tranca S, Cocis M, Antal O. Lethal case of Vipera berus
bite. Clujul Med 2016; 89(3): 435–7.
- “Torlak” Institute of Virology, Vaccines and Sera, Belgrade,
Serbia. User’s manual for Viekvin®:
www.torlakinstitut.com/pdf/Viekvin-en.pdf
- Nikolić S, Simović A. First report on a trichromatic lowland
Vipera berus bosniensis population in Serbia. Herpetol Conserv
Bio 2017; 12(2): 394–401.
- Anonymous. Pravilnik o odštetnom cenovniku za utvrđivanje
visine naknade štete nedozvoljenom radnjom u odnosu na strogo
zaštićene i zaštićene divlje vrste [Regulation on the
compensation charges for the damages caused by illegal actions
towards strictly protected and protected wild species]. Službeni
glasnik Republike Srbije 2010; No. 37/2010.
- Stahel E, Wellauer R, Freyvogel TA. Vergiftungen durch
einheimische Vipern (Vipera berus und Vipera aspis). Eine
retrospektive Studie an 113 Patienten [Poisoning by domestic
vipers (Vipera berus and Vipera aspis). A retrospective study of
113 patients]. Schweiz Med Wochenschr 1985: 115(26): 890–6. [In
German with abstract in English]
- Warrell DA. Treatment of bites by adders and exotic venomous
snakes. BMJ 2005; 331: 1244.
https://doi.org/10.1136/bmj.331.7527.1244
- Malina Т, Schuller P, Krecsák L. Misdiagnosed Vipera
envenoming from an unknown adder locality in northern Hungary.
North-West J Zool. 2011; 7(1): 87–91.
|
|
|
|